
| The University of Connecticut School of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Statements of credit for the online activity ACPE UAN 0009-0000-26-005-H01-P/T will be awarded when the post test and evaluation have been completed and passed with a 70% or better. Your CE credits will be uploaded to your CPE monitor profile within 2 weeks of completion of the program. |
Content
INTRODUCTION
Let’s start this continuing education (CE) activity with a case. Bob is a 63-year-old who has had lifelong exacerbations of disabling psychosis. In addition to his psychiatric diagnosis, Bob also struggles to control concomitant medical conditions. These conditions include urinary incontinence, benign prostatic hyperplasia (BPH), and severe constipation that persists from a previous gastrointestinal obstruction and surgical perforation. He has been experiencing breakthrough psychotic symptoms on his current antipsychotic and arrives at the pharmacy today to pick up his new antipsychotic, xanomeline combined with trospium chloride (Cobenfy). Bob mentions to the pharmacy technician he is also having pain and trouble sleeping. He would like to purchase a bottle of over-the-counter (OTC) Tylenol PM (acetaminophen with diphenhydramine). The pharmacy technician recognizes diphenhydramine’s potential conflict with his new prescription and alerts the pharmacist. Staying current with new medications is key to providing optimal care and safety for patients. The pharmacist contacts the prescriber to discuss less complicating anticholinergic options for Bob.
Acetylcholine (ACh) is a neurotransmitter found in the brain and peripheral nervous system. Pharmacologic manipulation of this neurotransmitter has resulted in the advancement of novel pathways to treat conditions ranging from anaphylaxis rescue to treatment of dementia. Unintentional consequences of ACh manipulation include adverse effects associated with anticholinergic burden (ACB). The magnitude of ACB increases with the number of medications with anticholinergic characteristics added to the prescribed regimen. Often overlooked is the added burden of a patient’s OTC medications ranging from sleep aids to antidiarrheals.1 It is also important to differentiate anticholinergic action from drug-induced fluid depletion, like that expected with diuretics, which have no hallmark muscarinic effects.
Increased ACB results in short-term adverse effects like dry mouth, blurred vision, and urinary retention. It can also cause or contribute to long-term effects including dementia, worsening physical function, and increased risk of falls.1 The characteristics of anticholinergic reactions are easier to remember when understanding the normal function of muscarinic receptors at different sites in the body. The following symbolic descriptions can help you recall these effects2:
- Mad as a hatter (delirium, cognitive deficits)
- Blind as a bat (eye symptoms, blurry vision)
- Dry as a bone (decreased sweating/dry mouth/dry skin)
- Hot as a hare (elevated body temperature)
- Bloated as a toad (constipation)
- The heart runs alone (tachycardia)
- Full as a flask (urinary retention)
- Red as a beet (cutaneous vasodilation)
Clinicians (including pharmacists and technicians) can rank medications according to their ACB contribution and predict their cumulative effects.
PAUSE AND PONDER: What diagnoses and conditions may be worsened if patients are exposed to anticholinergic medications?
What Does the Beers Criteria Have to Say?
The American Geriatrics Society (AGS) Beers Criteria warns of diminished medication elimination as we age. Using highly anticholinergic medications is riskier in older adults, resulting in exaggerated adverse effects such as confusion, xerostomia (dry mouth), and anticholinergic toxicity. Even younger adults are at risk of long-term cumulative exposure to anticholinergic drugs that can lead to delirium (an acute, fluctuating disturbance in attention and awareness) and dementia (a chronic, progressive cognitive decline).1 In addition to central nervous system anticholinergics, Beers also recommends avoiding anticholinergic gastrointestinal antispasmodics and skeletal muscle relaxants because of questionable efficacy (Table 1).1
Table 1. Illustrative List of Potentially Inappropriate Medication Use in Older Adults1
| Organ system | Therapeutic category | Illustrative examples | Recommendations |
| Central nervous system
|
Antidepressants with strong anticholinergic activity, alone or in combination
|
TCA
• Amoxapine • Clomipramine • Desipramine • Doxepin > 6 mg/day • Imipramine • Nortriptyline
SSRI • Paroxetine |
Avoid
• Highly anticholinergic, sedating. • May cause orthostatic hypotension
Exception: Low-dose doxepin 6 mg/day or less is comparable to placebo |
| Antiparkinsonian medications with strong anticholinergic activity
|
• Benztropine (oral)
• Trihexyphenidyl |
Avoid
Treatment of drug-induced EPS: Not recommended for prevention or treatment of EPS due to antipsychotics
Treatment of Parkinson disease: More effective medications are available for the treatment of Parkinson disease |
|
| ABBREVIATIONS: EPS = extrapyramidal symptoms; SSRI = selective serotonin reuptake inhibitors; TCA = tricyclic antidepressants | |||
The Beers Criteria also includes potentially inappropriate medications (PIMS) for older adults that can worsen a condition or syndrome. Anticholinergic medication can exacerbate lower urinary tract symptoms, BPH, and glaucoma. Therefore, prescribers should avoid them in patients with these conditions.1 Peripheral effects of ACB include constipation, dry mouth, tachycardia, and urinary retention. Central adverse effects include agitation, confusion, delirium, and cognitive impairment. Individuals with serious mental illnesses (SMI) are in a state of chronic cerebral cholinergic depletion and exposure to high ACB can worsen negative symptoms (a reduction or absence of normal behaviors and functions related to motivation and interest, or verbal/emotional expression) leading to further functional and cognitive impairment.3
Anticholinergic medications frequently cause dry mouth, and medication-induced xerostomia can result in discomfort and oral health complications.4 Saliva not only facilitates swallowing and digestion, but also promotes the removal of harmful microorganisms.5 Medication-induced xerostomia has been reported in twice the number of patients taking anticholinergic medications compared to non-medicated individuals (30% as opposed to 16%, respectively).6 Data suggests that patients with dry mouth are 11.5% more likely to develop oral candidiasis, also called thrush, than those without xerostomia.7,8 More than 95% of dry mouth cases reported in residential long-term care settings for older adults were attributed to medication use and not a natural consequence of aging.4,9
The development of dementia with long-term anticholinergic use has been well researched. Numerous studies have investigated the potential cognitive impacts of prolonged chronic anticholinergic exposure.10-14 Epidemiological research has demonstrated that anticholinergic medications’ impact on the development of dementia is significant, with an increased risk of up to 50% among those with high ACB. Researchers have been able to detect risk associated with anticholinergic use up to 20 years before diagnosis.10-14
PAUSE AND PONDER: What diagnoses and conditions may be affected when using anticholinergic medications? What OTC medications may pose anticholinergic risk?
ESTABLISHING AN ACB ACTION PLAN
Establishing an ACB action plan is as easy as following five steps.
First, the Beers Criteria expert panel recommends routine medication reviews that include consideration of total ACB. Clinicians should calculate ACB risk scores to determine ACB magnitude. Numerous published scales are available to measure ACB. Expert consensus groups develop scales using clinical experience along with research evaluating anticholinergic properties of medications. One calculator that is available is the ACB Calculator, which combines the Anticholinergic Cognitive Burden Scale (ACBS)15 and the German Anticholinergic Burden Scale (GABS).16 This calculator is available at https://www.acbcalc.com/.17 The developers report their source calculators are valid, reliable, and have been used as a pharmacology standard to measure ACB. A score of 3 or greater on the ACBS is associated with significant cognitive impairment and increased mortality.
The second step is to use direct observation and consider patient self-reported adverse effects.
- Clinicians should inquire about physical symptoms associated with anticholinergic toxicity at each patient encounter. They should evaluate ACB in individuals with new or worsening urinary retention, significant constipation, dry mouth, or any of the symptoms described earlier.
- Clinicians should evaluate individuals who report confusion or new or worsening memory impairment for ACB.

Third, the clinical team needs to evaluate the patient’s regimen to determine whether pharmacologic substitution to medications with less ACB is possible.
- Diphenhydramine (Benadryl) or sedating antihistamines for allergies? Individuals seeking relief of allergic symptoms may find less sedating options such as loratadine (Claritin) adequate. For others requiring greater control, exploring intranasal steroids (like fluticasone) used along with loratadine may provide better symptom relief.
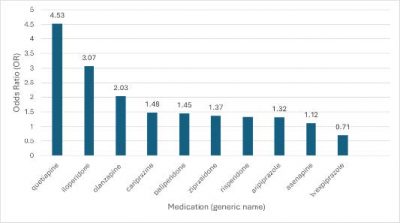
- Ask the question, “Can the patient use antipsychotics or antidepressants with less ACB?” Individuals taking antipsychotics report a spectrum of adverse effects and symptom improvement. Clozapine is ranked among the most anticholinergic antipsychotics currently available, however its position also as the most superior antipsychotic prevails for many patients who need it.18 Clinicians can evaluate potential ACB using established rankings when prescribing antipsychotics. Odds ratios reveal that quetiapine (Seroquel) has one of the highest odds ratios of 4.53, meaning a 4.53 times higher chance of experiencing anticholinergic effects (see Figure 1).18 While not all antipsychotics are entirely interchangeable, evidence supports relative equivalency for most when given for an adequate duration and at optimal doses. Antidepressants can be ranked for ACB more efficiently by their class effects, with the tricyclic antidepressant class contributing high ACB and selective serotonin reuptake inhibitors (SSRI)/serotonin norepinephrine reuptake inhibitors (SNRI) with low ACB contribution potential. The SSRI paroxetine (Paxil), however, is an exception to the SSRI class benefit because Beers cautions against its use for those at risk of high ACB.1
Figure 1. Anticholinergic Effects of Commonly Prescribed Second Generation Antipsychotics Ranked by Odds Ratio18
Fourth, it’s essential to educate patients about OTC medications for sleep and allergies that have anticholinergic properties.1,19
- Using diphenhydramine in situations such as acute treatment of severe allergic reactions is appropriate, even for older adults. Having diphenhydramine on hand for many families is critical to emergency planning.
- Diphenhydramine and other sedating antihistamines are limited by tolerance that develops when used chronically as a sleep aid. Melatonin is a popular alternative; however the Food and Drug Administration (FDA) regulates it less strictly than other medications, and some formulations contain inconsistent amounts of melatonin. In fact, analysts have found melatonin supplements to contain almost 3.5 times more melatonin than reported on the label. Prescription melatonin agonists like ramelteon (Rozerem), are an option for individuals who prefer a non-controlled, FDA approved intervention for sleep onset insomnia.
- Patients with sleep complaints can try nonpharmacologic interventions before exploring medications that can cause further complications. Interventions include developing a consistent schedule for sleep-wake times, controlling the environment (decreasing noise and temperature), and avoiding vigorous physical activity and caffeine consumption before bedtime. Avoiding blue light from cell phones and other devices is also essential to promote natural melatonin release and facilitate decreased sleep latency.
- Pharmacy technicians can be a great to deliver educational materials with pharmacist review. These materials can include symptom checklists prepared by healthcare professionals. Pharmacists should calculate scores when a patient presents with possible ACB or when conducting a routine medication review. Pharmacists can also check ACB scores technicians calculate for them before they share them with patients. Pharmacy technicians be sure to include OTC purchases and all prescription medications because burden scores should consider the total medication regimen.
Finally, all healthcare providers need to stay current with newly approved medications because these may not be available in an ACB calculator.1,20
- The AGS Beers Criteria is scheduled for updates every three years. Pharmacists and pharmacy technicians should review the summary tables that highlight anticholinergic agents newly included in the List.
- ACB calculators are limited by the medications they include for ranking. New medications are often not readily available until expert update the calculator.
- Cobenfy’s prescribing information, for example, is not available in the ACBS yet. This “first in class” antipsychotic is a muscarinic combination of xanomeline and trospium chloride. The prominent precautions provided in its labeling are associated with its anticholinergic adverse effects and risks, as reflected in Table 2.
Table 2. Highlights of Xanomeline/Trospium Chloride’s Anticholinergic Warnings20
| Contraindicated in patients with
|
• Urinary retention
• Moderate or severe hepatic impairment • Gastric retention • History of hypersensitivity to xanomeline or trospium chloride • Untreated narrow-angle glaucoma |
| Clinical Considerations
|
• Risk of urinary retention: can cause urinary retention.
• Biliary disease: Assess liver enzymes and bilirubin prior to initiating and as clinically indicated (with caution). • Symptoms of gallbladder disorders, biliary disorders, and pancreatitis should be assessed as clinically indicated during treatment. • May decrease gastrointestinal motility: Use with caution in patients with gastrointestinal obstructive disorders because of the risk of gastric retention. • Risk of use in patients with narrow-angle glaucoma: Use only if benefits outweigh the risks and with careful monitoring. • Increases in heart rate: May increase heart rate (monitor) |
So, what about Bob? Clinicians skilled in developing ACB action plans determined that with some small changes, as described in Table 3, they could minimize his anticholinergic risks. They continued some of Bob’s current medications that did not contribute to the ACB. More options could be considered in the future if Bob’s symptoms continue or require further intervention. For example, the clinical team chose brexpiprazole because it had the least ACB of available options, but many others could be explored. What changes would you have made?
Table 3. Reducing Bob’s Anticholinergic Burden
| Bob’s medication list | ACB score
currently |
Action | Alternative | ACB score recalculated |
| Oxybutynin for urinary incontinence | 3 | Choose alternative | Mirabegron | 0 |
| Quetiapine for psychosis | 3 | Choose alternative | Brexpiprazole | 0 |
| Acetaminophen with Diphenhydramine for insomnia and arthritis pain | 0
3 |
Choose alternative | Plain APAP
Ramelteon for sleep onset insomnia |
0
0 |
| Tamsulosin for BPH | 0 | No change | 0 | |
| Total ACB score | 9 | 0 | ||
| ABBREVIATIONS: ACB = anticholinergic burden, BPH = benign prostatic hyperplasia | ||||
CONCLUSION
Clinicians should consider using a calculator, such as the Anticholinergic Burden Calculator, as a clinical support tool for determination during a routine medication review. Many medications with anticholinergic properties are prescribed out of clinical necessity and without an appropriate alternative for certain patients. Calculating ACB is also advisable if the patient presents with symptoms that suggest possible anticholinergic toxicity.