Learning Objectives
After completing this application-based continuing education activity, pharmacist preceptors will be able to
| 1. Describe professional identify formation |
| 2. Apply the steps in development of a professional identity |
| 3. Identify activities that develop professional identity appropriately |

Release Date: February 23, 2026
Expiration Date: February 23, 2029
Course Fee
Pharmacists: $7
UConn Faculty & Adjuncts: FREE
There is no grant funding for this CE activity
ACPE UANs
Pharmacist: 0009-0000-26-016-H04-P
Session Code
Pharmacist: 23PC49-ABC37
Accreditation Hours
2.0 hours of CE
Accreditation Statements
| The University of Connecticut School of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Statements of credit for the online activity ACPE UAN 0009-0000-26-016-H04-P will be awarded when the post test and evaluation have been completed and passed with a 70% or better. Your CE credits will be uploaded to your CPE monitor profile within 2 weeks of completion of the program. |
Disclosure of Discussions of Off-label and Investigational Drug Use
The material presented here does not necessarily reflect the views of The University of Connecticut School of Pharmacy or its co-sponsor affiliates. These materials may discuss uses and dosages for therapeutic products, processes, procedures and inferred diagnoses that have not been approved by the United States Food and Drug Administration. A qualified health care professional should be consulted before using any therapeutic product discussed. All readers and continuing education participants should verify all information and data before treating patients or employing any therapies described in this continuing education activity.
Faculty
Jennifer Luciano, PharmD
Director, Office of Experiential Education; Associate Clinical Professor
UConn School of Pharmacy
Storrs, CT
Jeannette Y. Wick, RPh, MBA, FASCP
Director, Office of Pharmacy Professional Development
UConn School of Pharmacy
Storrs, CT
Ethan Yazdanpanah
PharmD Candidate 2025
UConn School of Pharmacy
Storrs, CT
Faculty Disclosure
In accordance with the Accreditation Council for Pharmacy Education (ACPE) Criteria for Quality and Interpretive Guidelines, The University of Connecticut School of Pharmacy requires that faculty disclose any relationship that the faculty may have with commercial entities whose products or services may be mentioned in the activity.
Jeannette Wick, Ethan Yazdanpanah, and Jennifer Luciano do not have any relationships with ineligible companies
ABSTRACT
Discovering what it means to be a good healthcare provider goes beyond knowledge acquisition and education for pharmacy students; it demands a transformative journey of professional identity formation (PIF). The pharmacy profession, through its professional organizations, has identified a number of core values, but as the profession changes, new core values are emerging. PIF occurs over a trajectory, starting in pharmacy school (or even before) and continuing throughout life. Preceptors can use a number of techniques to help pharmacy students with PIF, assuring that our future pharmacists hold the same values ats the profession at large. Exposing students to a variety of situations, asking open-ended questions, using teach-back methods, and introducing students to professional organizations are a few.
CONTENT
Content
INTRODUCTION
Let’s begin this continuing education activity with some questions. What makes a nurse a nurse? What makes a nurse a good or exceptional nurse? What makes an electrician an electrician? What makes an electrician a good or exceptional electrician? What makes a pharmacist a pharmacist? What makes a pharmacist a good or exceptional pharmacist? Those questions are no doubt difficult to answer. Preceptors may be making a list mentally of the qualities that the ideal nurse, electrician, or pharmacist should possess. Certainly, for each of these professions, education will be the foundation. Here’s a harder question: Is it possible to be a good or exceptional nurse, electrician, or pharmacist but a terrible person? And is it possible to be a good and loyal pharmacy employee, but not such a good pharmacist? All these questions speak to the concept discussed here: professional identity.
Discovering what it truly means to be a healthcare provider goes beyond knowledge acquisition and education for pharmacy students; it demands a transformative journey of professional identity formation (PIF) starting even before introductory pharmacy practice experiences (IPPE) (perhaps with acceptance into a pharmacy program or during professionalism ceremonies) and continuing past graduation and over an entire career. As the introduction hints, preceptors must distinguish between education, professionalism, and professional identity. A quick way to differentiate between the latter two is that a student’s professionalism is outwardly observable. Professional identity, however, is defined by a student’s internal thinking, feeling, and acting like a member of the pharmacy profession and its community.1
Pharmacists can use their extensive, science-based education to assume many professional identities; they may work in community, hospital, health-system, research, information technology, marketing, or a vast number of other positions. Viewing the history of the profession in just the last century, various identities have accumulated (rather than shifted) over time.2 The typical pharmacist’s main responsibility was once compounding. As the industrial revolution made it possible to produce dosage forms en masse, compounding fell out of favor and dispensing manufactured products became the primary focus of a typical pharmacist. Within just the last 20 years, pharmacists have made major inroads into establishing their role as necessary health care professionals rather than just retailers.3 Pharmacists have been shown to be key in improving therapeutic outcomes with a new focus on patient focused intervention.4 Pharmacists’ employment opportunities are growing and adapting to a changing field but the profession’s fundamental or core values are somewhat fixed. Table 1 lists the pharmacy profession’s current core values as promulgate by the American Pharmacists Association.
Table 1. The Pharmacist’s Core Values5,6
| Commitment to the patient’s well-being | · Engage in shared decision making and respect patients’ right to self determination
· Protect patient life and aim for best outcomes |
| Pharmaceutical expertise | · Maintain competence in knowledge and abilities to ensure the safe and effective use of medication |
| Reliability and care | · Find balance between risk and benefit in treatments
· Maintain trust and confidentiality with patients · Collaborate reliably with other healthcare professionals to ensure best health outcomes |
| Social responsibility | · Act with honesty and integrity in professional relationships
· Avoid discrimination and seek healthcare equity in society |
PAUSE AND PONDER: Look at Table 1. What other values would you add to the table?
As the profession’s identity evolves, pharmacists’ identities and their core values must follow suit. While pharmacists must be lifelong learners and adapt over time to new conditions, change is most readily achieved in the initial learning process as pharmacy students. In other words, you can teach old dogs new tricks, but it’s easier to teach puppies. In class, faculty teach students information a pharmacist should know and address how to outwardly act like a professional, but the profession demands something more: the development of a professional identity. We rely on our community of pharmacist preceptors to augment the various didactic courses to cultivate new pharmacist graduates who identify strongly with our core values.
PIF is a crucial aspect of pharmacy experiential education. Students require experiential learning and immersion into the profession to assimilate the qualities that make pharmacists unique and different from other healthcare providers. The Accreditation Council for Pharmacy Education (ACPE)-required IPPE rotations provide students with important opportunities to influence PIF, and the PIF process continues during a student’s advanced pharmacy practice experiences (APPE).7
The Pharmacy Student’s IPPE Rotation
IPPE rotations serve a much broader purpose than students fulfilling educational requirements and completing dreaded 50-page workbooks that some schools use that aim to help them reflect on or consolidate learning. IPPE rotations should introduce students to the way front line pharmacists navigate real-world pharmacy practice situations. Students primarily relegated to counting pills and organizing stock in the back of a pharmacy are unlikely to develop professional identities. If students perceive that preceptors think of them as free labor or burdensome obligations, they will not engage in the deeper discussions about the preceptor as a person fulfilling professional obligations. Students should observe and actively take part in various aspects of the profession, applying theoretical knowledge acquired in classrooms to real-world situations. Practical knowledge gained through these experiences helps students to develop essential professional skills and test their learning.
Experiential learning rotations should also expose students to different types of pharmacist positions and responsibilities. By observing different practice settings and interacting with pharmacists, patients, and other healthcare professionals, students can explore their interests, while realizing their strengths and developing professional values.
Step-by-Step to Professional Identity
Throughout pharmacy education, faculty members encourage students to exhibit professionalism; they may
- suggest more productive ways to present ideas
- prompt students to elevate or refine language or speak in ways patients will understand, or
- suggest that certain clothing choices can diminish peoples’ view of them and their credibility
While classroom faculty can teach and model the concept of professionalism, preceptors have the responsibility of supporting students in their PIF journey. Teaching starts the learning process; ultimately, students will need to “create their own adventures.” In other words, they must learn to apply aspects of specific material and explore different experiences to develop a professional identity. Relating to the definition of PIF, a pharmacy student’s PIF process must involve thinking, feeling, and acting like a pharmacist.
To discuss professional identity, preceptors and all pharmacists who influence the student’s learning process must acknowledge the steps inherent in PIF. Personal identity is based on an individual’s concept of who they are and how others perceive them.7 Individuals develop personal identity in stages starting at birth but personal identity begins at birth and continues throughout life. Professional identity develops in a similar but slightly different way.
Robert Kegan, a Harvard psychologist, developed a framework for longitudinal development of the self into a moral meaning-making entity that has had lasting impact on PIF in education of professionals.3,8-10 His framework includes six stages with stage 0 beginning at birth. Stages 0 and 1 concern young children’s development of basic motor function and sensing the physical world around them (and are not discussed here).8
In relation to PIF, the health professional must pass through at least stages 2 through 4 of the framework: imperial, interpersonal, and institutional.10 This framework, with steps 2 through 5 shown in Table 2, defines the personal characteristics and related professional context of an individual in continuous stages of development. Individuals who reach the final stage, stage 5, or the inter-individual self-transforming stage, open themselves to multiple identities and other value systems, achieving full personal autonomy.8 Research shows that not all individuals reach stage 5.10,11 However, with effective socialization partnered with experience in the pharmacist’s potential identities, students may reach this level during their careers.
Table 2. Kegan’s Stages of Personal and Professional Identity Development8,10
| Stage | Personal characteristics | Professional context |
| 2. Imperial | Individuals put their own needs and interests first but consider other people’s views. | Individuals fill their professional roles but do so with a primary motivation of following rules. Individuals exhibit low self-reflection and may struggle to balance emotions with reason. |
| 3. Interpersonal | Individuals are concerned with others’ perceptions of them and able to reduce focus on self-interest. Individuals balance multiple perspectives simultaneously. | Individuals are idealistic and self-reflective, seeking others to guide them. Individuals manage emotions acceptably and generally understand right and wrong. |
| 4. Institutional | Individuals assess relationships with a focus on self-defined principles and standards. Individuals define themself independently of others. | Individuals can understand relationships by appreciating different values and expectations. They internalize professional values and do not allow emotion relating to needs, desires, and passion to gain control over reason. |
| 5. Self-transforming | Individuals reconcile contradictory or paradoxical ways of constructing meaning. They can recognize the interdependencies of different systems or ways of thinking. | The self-transforming professional has a strong sense of self but also relies upon others knowledge and opinion in professional development. The professional integrates other identities into the total professional identity. |
The constantly evolving pharmacy profession and the lack of a specific list of steps for PIF makes it challenging for students to define an identity (and preceptors to help them). As the profession continues to develop to offer a wide range of opportunities for pharmacists, preceptors will observe students finding varying paths of PIF. Different pharmacists will define the profession differently depending on their experiences. Pharmacy students might generally navigate this list of steps, common among many young people developing professionally12-15:
- Exploration: In any career path, exploration is the first step in PIF. In pharmacy, the American Pharmacists Association offers the Career Pathway Evaluation (https://www.pharmacist.com/Career/Career-Pathways) to help aspiring pharmacists find a path forward. IPPE and APPE rotations should ideally provide students with opportunities to explore various pharmacy practice settings and work with pharmacists with a range of responsibilities. Students need to augment their existing identities—formed by their upbringing and personal beliefs—as they begin their pharmacy education and careers. Students come from diverse backgrounds with varying past experiences, cultural values, learning styles, and personal characteristics.
- Reflection and integration: Educators should encourage students to reflect on their experiences, strengths, values, and areas for improvement. Reflection helps students align personal and professional values, shaping their professional identities. Self-reflection and reflection from preceptors during IPPE rotations is necessary for growth. For example, a technician told Jayne, a pharmacist for a chain pharmacy, that a patient was in the counseling room and ready for an immunization. Jayne took her student with her to observe. Jayne asked the student to review the necessary paperwork and make sure the patient, a 17-year-old adolescent, met all the criteria for the human papilloma virus vaccine. The student said he did. When Jayne reviewed the paperwork, she found one problem. She asked the patient, “Which of your parents is here with you today?” In Jayne’s state, the legal age of consent was 18. When contacted by phone, the parent agreed to come in immediately and Jayne administered the vaccination. After all was done, she spent just a few minutes talking to the student about the duty to protect and comply with the law, describing a couple of other instances when she encountered similar situations.
- Commitment and advocacy: Commitment to the pharmacy profession and dedication to lifelong learning are essential elements in the development of a professional identity. Pharmacy students will become spokespeople for the profession and advocate for the inevitable change from retail-based to clinically- or service-based work. Pharmacists with solid professional identities will be lifelong learners and educators.
Students who have never worked in a pharmacy or observed a pharmacist at work (and some who have) may have inaccurate ideas about the profession. Preceptor Eddie encountered a curious situation when Adam, a P2 student, reported for an IPPE rotation. Adam was more than self-assured; Adam had an exaggerated sense of self-worth. He was bumptious (self-important or smug), so Eddie needed to work around Adam’s personal identity. Adam told Eddie that his older brother was a pharmacist who had told him that pharmacy schooling is pretty worthless. Adam said, “All you need to do is pass and you’re on your way to a darned good salary.” Eddie was astounded. Adam needed help reaching Step 2 of the PIF model—he was putting his own needs and beliefs first and disregarding others’ views. Eddie created a plan to help Adam develop more insight.
Each day when Adam came to work, Eddie presented two or three situations from his work experience that required more than just a body behind a computer. He would ask Adam to work through the problems and present the answers by the end of the day. In this way, he educated Adam about professional responsibility and clarified the difference between a person with a pharmacy degree and an exceptional pharmacist. PIF’s goal is for students to move from playing or imagining the pharmacist’s role to internalizing the pharmacist’s identity and acting as pharmacists at the unconscious level. The process shifts emphasis from ‘doing’ to ‘being.’ While professionalism can be put on and taken off like a white coat, professional identity stays with the healthcare professional at all times. Eddie was able to improve Adam’s professionalism, which was poor at the rotations start, and contribute to Adam’s professional identity.
PAUSE AND PONDER: When you were a student, which preceptors influenced your core values and how did you internalize them?
Activities that Develop Professional Identity
Preceptors who work in different types of positions need to acknowledge their personal and professional strengths and limitations to determine what they can realistically offer to students. Before taking on the preceptor’s or mentor’s responsibilities, professionals must be familiar with their own skillsets.7,14
- The first step preceptors should take is to embrace self-reflection. Just as preceptors should encourage students to engage in reflective practice, pharmacy is a profession in which preceptors must be lifelong learners. Established pharmacists will continue to accumulate PIF-related experiences over time to aid their effectiveness in guiding others.
- Preceptors will then need to plan intentionally and commit to helping students develop professional identity. A reluctant or unprepared preceptor usually cannot teach students effectively. Sometimes pharmacists with extensive work experience on the frontlines might feel that students come with a more contemporary knowledge base and therefore, they have nothing to teach them. However, that pharmacist could be well-positioned to support the student’s PIF by embracing how their professional experiences led to a deeper understanding of their profession and the pharmacist’s role in supporting patient outcomes.
PAUSE AND PONDER: What are the most efficient ways to help your students develop professional identity in your practice location? What are the most important ideas you can teach? Are they the same?
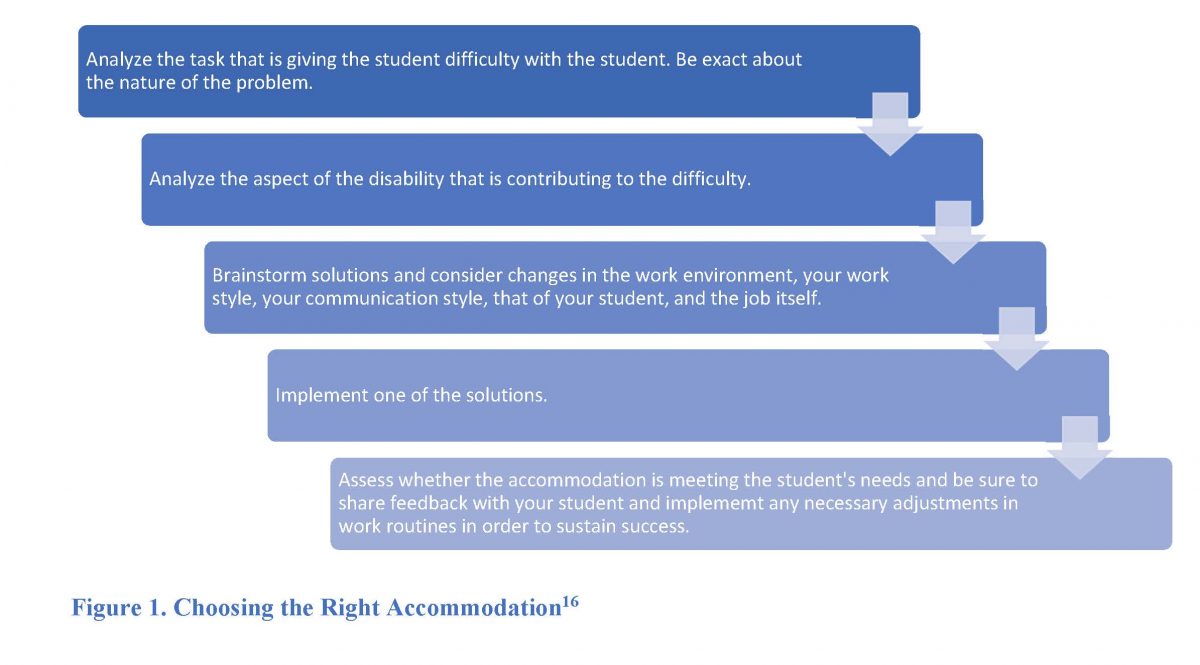
PIF is a gradual process that revolves around socialization, not classroom lecture. IPPE rotations provide an ideal platform for students to engage in activities that promote professional development. Preceptors can work with students to facilitate PIF during an IPPE rotation in several ways. 7,16,17
Patient interactions: Direct patient interaction during IPPE can help students apply theoretical learning and develop communication skills, empathy, and a patient-centered approach to care. These experiences help students internalize a sense of responsibility toward patient well-being and strengthen trust in the caregiver-patient relationship.
Preceptors should expose students to patient counseling sessions as observers as often as possible. Consider Leonard, a preceptor who frequently tells students, “I am not going to bring you into this counseling session because it is too complicated. You won’t understand what’s going on.” This is a mistake. IPPE is an opportunity for students to be exposed to difficult real-life examples before they have to handle them alone. These experiences help develop professional identity and may even stimulate an “ah-HA!” moment about pharmacist responsibility for the student. Preceptors who ask students a few open-ended questions (e.g., What did you see that surprised you? What three points did I emphasize? What counseling techniques will you remember from this?) prompt students to engage. Inviting students to see a situation that requires pharmacists to work at the top of their license introduces step 4 (institutional) and epitomizes PIF. Leonard has the opportunity to show his version of an independent and talented pharmacist who contributes to healthcare positively.
PIF opportunities need not be complicated. Sometimes PIF occurs concurrent with simple everyday tasks. Preceptors who walk students through their thought process when processing an order (i.e., Why does this document go here in the electronic medical record? Why am I looking at that lab before processing the order?) introduce students to the necessity of questioning routinely as a professional function. They can also ask students to find or calculate doses, explore drug interactions, and then provide the information to another interdisciplinary team member.
Not all patient interactions are pleasant or welcome, but they may be professionally necessary. Alex, the pharmacist, was dismayed when a technician came to him and said, “Mrs. Royce is here and wants to talk to you,” while rolling her eyes. Mrs. Royce was notorious for being loud, disrespectful, and a know-it-all. Alex didn’t answer immediately. The technician said, “Shall I tell her you are busy?” Alex said he would talk to her and briefed the IPPE student on Mrs. Royce’s personality. He said he was concerned because Mrs. Royce had recently had surgery, had a reaction to the opioid that was prescribed, and was switched to tramadol. He explained that regardless of his personal feelings, he needed to deal with the situation. When he asked Mrs. Royce how he could help her, she said, “The oxycodone made me sick as a dog. My friend up the street who is a nurse says the tramadol I am taking now is not worth anything. I am taking it and it is super mild but at least it’s something. I have an anti-inflammatory, too. I know this is a first-world problem since this was an elective surgery, so I should not complain. I am just a whiner with pain.” Alex reassured her that no one deserves pain, even if the surgery was elective. Alex counseled the patient with these points18-20:
- Tramadol is a funny drug. People with certain genetic variations called CYP2D6 deficiencies get less relief from it. It gets a bad reputation because many clinicians don't know that. Take it if it helps. And it sounds like it helps a bit.
- Schedule your anti-inflammatory around the clock. Don't wait until the pain is horrible. Take it every four to six hours for a few days. Eat a little something when you take it.
- Use warm or cold compresses if they help but use them only for 10 minutes at a time once every hour. (You don't want to fry or freeze your skin.) If warm helps, use warm. If cold helps, use cold.
- Move around as much as you can. It increases blood flow to the area.
- Have you tried some acetaminophen? Some people find that taking a couple of acetaminophen once or twice a day for a couple of days helps--it won't address the inflammation but it may help with pain.
- Consider finding an acupuncturist and/or a massage therapist who specializes in pain.
After the session, Alex explained that dealing with patients like Mrs. Royce is an obligation, as is not showing whether he likes her. This attitude aligns with the “interpersonal” step of PIF (step 3)—balancing multiple perspectives and putting others’ needs first. He said that all pharmacists encounter difficult patients. He also said that he planned to check in on her by phone the next day. He asked the student if anything surprised her, and she said, “Yes. You didn’t say anything about the nurse’s bad advice!” Alex explained that professionals don’t speak badly of each other, especially when the information from Mrs. Royce was hearsay. He said he trusts that Mrs. Royce, the consummate know-it-all, will talk to the nurse and the nurse will call if she wants more information. The student was able to teach-back the key points of professional identity:
- Treat all patients with respect, even when they don’t return the favor
- Counsel carefully
- Do not disparage other healthcare providers (talk to them directly if you have a concern about their advice)
- Follow-up.
When the student asked this preceptor for a letter of reference several months later, the preceptor said, “Remember Mrs. Royce? Her attitude is entirely different now. She’s kind and respectful when she comes in.”
Collaborative Practice: Preceptors can highlight interdisciplinary healthcare experiences, demonstrating teamwork, collaboration, and the ability to contribute effectively within a healthcare setting. In a health system setting, for example, many different pharmacists work in the same organization with varying responsibilities. A health system may include an inpatient and outpatient, specialized clinical, emergency department, investigational drug service, and oncology pharmacy. Each position requires modified professional identities and collaboration with different healthcare professionals. A preceptor can join forces with other pharmacists—a model that is increasingly popular and often called team precepting—to ensure students receive a well-rounded education in the short period of time provided.
Exposure to eustress (healthy, stimulating kind and level of stress): A preceptor should take the time to facilitate a learning environment that optimizes the likelihood that PIF will occur. Preceptors can discuss situations that present ethical dilemmas during IPPE rotations, prompting critical thinking, ethical decision-making, and the development of moral reasoning. As students are exposed to common ethical dilemmas, they will begin to develop problem solving skills; build confidence; and think, act, and feel like pharmacists. Students who have not yet assimilated the second step of PIF—the imperial—may be more concerned with packing up to leave at their assigned quitting time than finishing a task. Helping students learn that sometimes the clock should not dictate decisions also develops professional identity.
Exposure to unanticipated, stressful misadventure. Marguerite was precepting a student when a technician came behind the bench with arms raised and a robber holding a gun behind her. The four other employees and the student froze, and Marguerite handled the situation, emptying the vault into the robber’s duffel bag. After the robbery, everyone was shaken but no one was hurt. Although the store manager’s opinion was to send the student home, Marguerite insisted on a post-incident stress debriefing. It gave everyone the opportunity to vent and identify what they did well and what they could do better, and reduced the likelihood of post-incident stress.21 As they met, the police returned and said they had apprehended the robber because Marguerite had placed a tracking device in the duffel bag. Marguerite has traversed all the steps of PIF. She considered others in her decisions, balanced multiple perspectives, and maintained her standards.
Although this is an extreme example that underscores the meaning of “unanticipated,” the student reported feeling better and understanding more about the pharmacist’s responsibilities. Other unanticipated events that can convey PIF include dealing with irrationally irate customers, diffusing the situation with a vaccine refuser who wants to espouse her opinion loudly to other patients, or dealing with a patient or employee medical emergency in the workplace. Appropriate and deliberate use of emotion can also focus learners and enhance learning, especially when the material is moving or highlights the patient’s perspective. Preceptors should employ emotion as a teaching tool carefully, since negative emotion (e.g., anger, embarrassment) erodes trust and can disenfranchise students.
Professional involvement: If time allows, preceptors can encourage students to engage with professional organizations. Attending conferences, workshops, state pharmacy board meetings, or seminars that promote professional growth, networking, and exposure to current trends in the pharmacy field builds professional identity. Preceptor Eddie, discussed previously, took Adam to a Board of Pharmacy meeting. Adam seemed uninterested until the Board discussed disciplinary action against a pharmacist who had failed to perform due diligence, leading to a patient’s death and a pharmacist with a drug abuse problem. Adam was less bumptious in the car on the way back to work, and Eddie took time to ask open-ended questions to mold Adam’s professional identity. He asked, “What questions do you have for me?” Adam said, “What is the chance they will get their licenses back?” It created a chance to talk about professional responsibilities and how state boards monitor and ensure public safety. Eddie asked a question of his own “What do you think the patients who experienced poor care or unprofessional behavior from those pharmacists think about the profession of pharmacy? In the world of social media, how far do you think those negative sentiments about pharmacists can spread?" This discussion moved Adam further through Step 2, and away from a preoccupation with self-interest.
Formative feedback (feedback that helps students recognize knowledge gaps and molds the student’s beliefs and values; see the SIDEBAR) and encourage reflection. Preceptors should7
- Provide students with regular feedback, but also schedule time for check-ins and reviews mid-rotation. As students’ professional identities develop, they will become their own sources of feedback.
- Employ teaching methods such as using teach-back and open-ended questions.
- Schedule time for students to work on workbooks or other tools for reflection and encourage discussion and questions.
- Assign meaningful work to help students integrate ethical principles, evidence-based practice, effective communication, and patient-centered care.
SIDEBAR: Formative Feedback22,23
Formative feedback
- refers to informal constructive feedback provided throughout a learning process
- is ongoing and proactive
- is specific and actionable
- helps to develop self-awareness and independence
- gives students the opportunity to reflect and adjust without being graded
- and is not summative feedback (a method of assessment where students are evaluated and/or graded on their overall performance usually at the end of a learning period)
Open ended questions are important in formative feedback. Just as healthcare professionals are encouraged to ask patients open-ended questions, preceptors should do the same with their students. Open-ended questions
- give students the opportunity to participate in discussion actively and gain a deeper understanding of a topic or situation
- can help the preceptor identify gaps in a student’s understanding
- develop students’ critical thinking skills and autonomy to further their PIF
- are especially useful after patient counseling or other interaction.
Teach-back, or the "show-me" method, confirms whether a person—a patient or in this case, a student—understands the topic being explained. Pharmacists and other healthcare providers use the teach-back in patient counseling to facilitate better communication between patient and provider. This tool allows a healthcare provider to assess patient understanding by having a patient explain, or teach-back, what they took away from the counseling session. The healthcare provider can gently correct misunderstandings. Using teach-back with students is especially effective when
- Students observe a complicated counseling session or process
- Students are learning about a new medical device or a medication with an unusual administration route or schedule
- Students need to research a topic that is new to them and may have missed some critical information
- Students witness a situation that is emotionally charged or creates a safety concern
Demonstrating vulnerability. Preceptors often want to hide their deficiencies, limitations, or weaknesses from students so students will have greater confidence in the preceptor’s expertise. Students need to see how mistakes happen and lead to improvement. They also need to see the ethical challenges that are inherent in pharmacy practice. Preceptor Terry received a phone call from a pharmacist who worked at another of her chain’s locations. She knew the pharmacist quite well, and the pharmacist said she had received a prescription for a patient well known to them for hydromorphone 8 milligrams. They were out of hydromorphone and the pharmacist asked if Terry had any 8 milligram tablets. Terry said she did, and the pharmacist said she would send the patient over and to expect him within 30 minutes. When the patient arrived, Terry filled the prescription and being alone with just the IPPE student, prepared to dispense it at the cash register. As required by law, she asked the patient for identification. Much to her surprise, the person presented his driver’s license and he was not the patient. In fact, the identification card was for the prescriber who had written the prescription, a medical resident at a local hospital. She asked the prescriber why he was picking up the prescription and he said that he was helping out the patient who was in terrible pain. It was late in the day, and Terry had received this referral from a colleague who she trusted. She dispensed the prescription despite her misgivings.
The next day when the IPPE student arrived, Terry explained the immediacy of the situation and conflicting professional interests led to dispensing the prescription yesterday, but she still had some nagging doubts. With the prescription volume a bit slower now, she decided to do some follow up. She found that the “patient” had a number of prescriptions filled over months, most of which were filled at her colleague’s pharmacy. However, the initial prescriptions were filled in a town 40 miles away. She eventually called the hospital, found the name of the residents’ supervising physician, and contacted him. After brief discussion, he indicated that he would handle it going forward and that he appreciated the information. Although the supervising physician did not say outright that he suspected this resident of wrongdoing, the implication was that was the case. The supervising physician did follow through and eventually, the state requested documentation. Terry was able to talk through the situation with the student and explain the pharmacist's responsibility in cases like this. Terry exemplifies Step 4 of PIF. She was secure in her identity and despite the way others had handled this situation, she was concerned and confident enough to do the right thing.
Teach-back is useful in many situations, but especially when processes are involved. In one busy pharmacy, a man approached the pharmacy student at counter. He said, “Can I get a shingles vaccine today?” The student, having no prior experience in a community pharmacy, politely asked the patient to wait while she asked the pharmacist. Her preceptor said quickly, “Get the patient’s insurance information and enter him into the system.” With the patient’s insurance card in hand, she began to enter his information. Unsure how to proceed, she asked the pharmacist for assistance again. A line began to form behind the man, so the pharmacist said, “Don’t worry, I’ll do it and you can watch.” The intern watched and thought the process looked easy enough. The pharmacist asked if she understands (a close-ended question), and she said yes. Later in the day, a new patient came in and the student began to enter the patient’s insurance information. She hit a point where she was unsure how to continue. But earlier she told her preceptor that she understood how to do it! She really thought she did know how! The student, becoming flustered, was embarrassed to ask for help again on something she had just learned. How could this situation have been avoided? If the preceptor had asked the student to describe the process, correcting any inaccuracies in recollection, and explained why pharmacies need to provide accurate information, the student would have been in a better position to help.
Overall, preceptors need to provide students with the best experience possible with available time and resources. For example, a student may be in a health systems rotation in a department that has little patient interaction and plenty of down time. The preceptor may worry he cannot give the student the experience she deserves. This preceptor could assign the student to review a journal article on a relevant subject and present it to an interprofessional team of nurses, pharmacists, and doctors. Subsequently, the student may realize the pharmacist’s potential impact and help the student internalize what it means to be a pharmacist.
PAUSE AND PONDER: Can you recall a time when you were taught how to do something, told your teacher you understood it, then could not perform the action on your own? As a preceptor, how would you avoid this situation with your own student?
Finally, let's return to the questions asked at the beginning of this continuing education activity. In particular, the question of whether a pharmacist can be a good employee, but a bad pharmacist, is of tremendous interest right now. The situation it brings to mind is that of the good employee pharmacist whose supervisors urge him to dispense opioid prescriptions as written and avoid asking too many questions. Doing so makes customers happy, increases prescription volume, and reflects positively in the store’s metrics. Many pharmacists conducted themselves this way for many years, despite the fact that they probably had an inkling that they should be checking more closely or perhaps turning some prescriptions away. These pharmacists were not necessarily bad pharmacists, but their employers considered them good employees because they followed directions and turned a blind eye to a developing opioid epidemic.
In November 2021, a federal jury in Ohio found three of the nation's largest pharmacy chains liable for contributing to the U.S. opioid crisis.24,25 The jury found that the prosecution provided ample evidence that some medications dispensed at chain pharmacies legally were sold on the black market. That finding has resonated nationally as state after state filed similar lawsuits. In December of 2022, two chain pharmacies agreed to share a $10.7 billion fine to settle allegations that they failed to oversee opioid analgesic prescriptions adequately. These funds are being distributed to states, local governments, and federally recognized tribes to improve opioid crisis abatement and remediation programs. Both chains agreed to improve their controlled substance compliance programs and provide mandatory training to pharmacists. Expediency in the short term and compliance with procedures that are unethical seldom avoid long term consequences.
Other states have also secured settlements from pharmacies, and independent pharmacies have also been prosecuted. Discussing situations related to pharmacy that appear in the media is another way that preceptors can introduce discussion of our professional values. The nation is hopeful that pharmacists everywhere have learned that part of our professional identity is the necessity to speak up and to challenge our employers when they ask us to do things that walk the line of professionally ethical behaviors. Starting discussions with students about newsworthy events like this in which preceptors talk about self-interest, other people’s perception of pharmacy and pharmacists, and maintaining standards can advance our profession. Pharmacists are part of a complex system of drug distribution. We need to establish our core values and uphold them to keep society’s respect.
CONCLUSION
Pharmacy educators, preceptors, and mentors must realize the significance of IPPE and APPE rotations and their influence in shaping future pharmacists’ professional identities. Professional identity formation is essential for students’ transformation into successful and compassionate pharmacists. IPPE rotations with effective preceptors enable students to observe, participate, and reflect on various aspects of pharmacy practice. Often these exercises take very little time, and small actions can have tremendous impact. Through exploration, reflection, and commitment to the profession, students can develop professional identities that align with the core values and beliefs of the pharmacy profession and their own personal values.
As students grow throughout their educational and professional careers, they will internalize what it means to be a pharmacist. Changes may not be apparent in the short amount of time a preceptor is with a student. If students are comfortable with the idea, preceptors can connect with them on LinkedIn, stay in contact through email, and be open to being a mentor to the student after the rotation ends. Pharmacy is a profession of many interconnected individuals with unique and valuable professional identities.
Pharmacist Post Test (for viewing only)
Who are you? Who are We? Professional Identity in Experiential Learning
Post-test
After competing this continuing education activity, preceptors will be able to
● Describe professional identify formation
● Apply the steps in development of a professional identity
● Identify activities that develop professional identity appropriately
1. Lyle is a preceptor whose student arrives to work wearing a tee shirt with a silly slogan on it, a ball cap, and brightly colored foam clogs. The student puts on a wrinkled and somewhat dirty white coat and steps out behind the register to start helping patients in the line. What is Lyle’s main concern with regard to this student?
A. Professionalism
B. Cleanliness
C. Professional identity
2. As the end of the day approaches, a prescriber calls in a set of prescriptions for a child who has a serious infection. Lyle assigns his student to check the dosing. The student asks if he can do the task tomorrow morning, as it's late and he'd like to head home for dinner. He also says that the prescriber probably double checked her own work. What is the BEST way for Lyle to explain the importance of completing the task today?
A. Explaining that one never knows when a patient will arrive to pick up prescriptions and how that reflects on the pharmacy staff. He is trying to help develop the student’s professionalism.
B. Explaining that most prescribers rarely double check their own work so the pharmacy needs to do it before the prescriber leaves for the day. This encourages professional identity formation.
C. Explaining that pharmacists have a duty to be diligent about medication doses, especially in pediatric patients. This should contribute to the student’s professional identity formation.
3. Mr. Walker, a patient who has successfully overcome an addiction to heroin, presents a prescription for oxycodone after having dental work. He wants to talk to the pharmacist, and you invite your student to join you. Mr. Walker asks if the prescription is for an addictive substance and says that the dentist never asked if he had a current or previous addiction problem. He would like you to call the dentist and have the prescription changed. You agree, and when you return to the pharmacy, your student asks, “Why don't you have him call the dentist himself? We're really busy.” What part of the pharmacist core values should you discuss with this student?
A. Pharmaceutical expertise
B. Commitment to the patient’s well-being
C. Social responsibility
4. Which of the following describes Step 2 in Kegan’s Stages of Personal and Professional Identity Development?
A. A student's primary concern is understanding others’ values and expectations.
B. A student's primary concern is ensuring the team approves of her work.
C. A student’s primary concern is in learning and following the rules of dispensing.
5. Which of the following accurately represents the sequence in which students can be expected to develop professional identity?
A. Learning the rules of pharmacy; learning to differentiate between right and wrong and working with other team members; removing emotion and using reason to make decisions
B. Learning to differentiate between right and wrong and work with other team members; removing emotion and using reason to make decisions; learning the rules of pharmacy
C. Removing emotion and using reason to make decisions; learning the rules of pharmacy; learning to differentiate between right and wrong and work with other team members
6. Which of the following accurately describes PIF opportunities in the pharmacy?
A. Preceptors who take IPPE students should use the simplest of examples to help students with PIF because students have little experience.
B. Preceptors should concentrate on situations that are complex so that students see pharmacists practicing at the top of their licenses.
C. Preceptors can use simple everyday tasks to help students understand the pharmacist's role and develop their professional identities.
7. Which of the following activities would be MOST appropriate for an IPPE student who has never worked in a pharmacy with regard to professional identity formation?
A. Having the student observe a controlled substance inventory and asking questions like, “Why do you think we conduct an inventory every day? What would we do if we found a discrepancy?”
B. Having the student observe a technician who is running the cash register and coaching the technician to ask questions like, “Do you have any experience running a cash register or dealing with customers?”
C. Having the student restock the OTC section of the pharmacy and make a list of OTCs that need to be ordered, and asking the student to justify her reasons for ordering the various drugs and the quantity she designates.
8. Which of the following activities is MORE appropriate for an APPE student than an IPPE student to develop professional identity?
A. Reviewing the case of a patient with drug resistant tuberculosis and several drug allergies and presenting the case on medical rounds with physicians and nurses
B. Checking that the dose of amoxicillin for a 5-year-old child who weighs 36 pounds is correct and that the child has no allergy to penicillin antibiotics
C. Asking the student to shadow you while you provide counseling to a patient who has a question about OTC cough and cold formulations
9. A new IPPE student has a casual attitude about pharmacy and expresses opinions that indicate that she knows very little about professional responsibilities. Several times and despite gentle correction, she has counted controlled substances incorrectly and returned control substance bottles to the regular shelves, not the vault. Which of the following activities might increase her awareness of the pharmacist’s responsibilities and legal obligations?
A. Having the student accompany you to your state’s Board of Pharmacy meeting
B. Abandoning formative feedback and pointing out the student’s errors forcefully
C. Restricting this student’s activity to handling the front end of the store only
10. Your state announces that it will now impose significant restrictions on all prescriptions for a certain drug because of a growing number of patient deaths related to its abuse. During the morning huddle, your staff discusses the increased paperwork burden and the potential that patients will be upset. After the huddle, the student asks, “Why is this our problem? Shouldn't this be handled by the drug’s manufacturer?” What is the best answer?
A. Technically pharmacists are nothing more than the medication police. Our job is to enforce the rules other create strictly and unemotionally.
B. In an ideal world, pharmaceutical companies would take complete responsibility for the damage their drugs do. This is not an ideal world.
C. Pharmacists are part of a complex system of drug distribution. We need to establish our core values and uphold them to keep society’s respect.
References
Full List of References
REFERENCES
1. Larose-Pierre M, Cleven AJ, Renaud A, et al. Reevaluating core elements of emotional intelligence in professional identity formation for inclusion in Pharmacy Education. American Journal of Pharmaceutical Education. 2023;87(6):100082. doi:10.1016/j.ajpe.2023.100082
2. Kellar J, Paradis E, van der Vleuten CPM, oude Egbrink MGA, Austin Z. A historical discourse analysis of Pharmacist Identity in Pharmacy Education. American Journal of Pharmaceutical Education. 2020;84(9). doi:10.5688/ajpe7864
3. Jarvis‐Selinger, S., Pratt, D.D., and Regehr, G. (2012). Competency is not enough: integrating identity formation into the medical education discourse. Academic Medicine 87: 1185
4. Toklu HZ, Hussain A. The changing face of pharmacy practice and the need for a new model of pharmacy education. J Young Pharm. 2013;5(2):38-40. doi:10.1016/j.jyp.2012.09.001
5. Kruijtbosch M, Göttgens-Jansen W, Floor-Schreudering A, van Leeuwen E, Bouvy ML. Moral dilemmas reflect professional core values of pharmacists in community pharmacy. Int J Pharm Pract. 2019;27(2):140-148. doi:10.1111/ijpp.12490
6. https://www.ashp.org/-/media/assets/policy-guidelines/docs/endorsed-documents/code-of-ethics-for-pharmacists.ashx
7. Johnson JL, Arif S, Bloom TJ, Isaacs AN, Moseley LE, Janke KK. Preparing pharmacy educators as expedition guides to support professional identity formation in Pharmacy Education. American Journal of Pharmaceutical Education. 2023;87(1). doi:10.5688/ajpe8944
8. Kegan, R. (1982). The Evolving Self: Problem and Process in Human Development. Cambridge, MA: Harvard University Press
9. Irby, D.M. and Hamstra, S.J. (2016). Parting the clouds: three professionalism frameworks in medical education. Academic Medicine 91: 1606–1611
10. Swanwick T, Forrest K, O’Brien BC, Cruess RL, Cruess SR. The Development of Professional Identity. In: Understanding Medical Education: Evidence, Theory and Practice. Wiley-Blackwell; 2019:239-254.
11. Hafferty, F.W. (2016). Professionalism and the socialization of medical students. In: Teaching Medical Professionalism (ed. R.L. Cruess, S.R. Cruess and Y. Steinert), 54–68. Cambridge: Cambridge University Press.
12. Briceland LL, Martinez T. Exploring the impact of reflecting upon pharmacy experts’ written career guidance on Student Professional Identity Formation. INNOVATIONS in pharmacy. 2022;13(3):5. doi:10.24926/iip.v13i3.4778
13. Arnoldi J, Kempland M, Newman K. Assessing student reflections of significant professional identity experiences. Currents in Pharmacy Teaching and Learning. 2022;14(12):1478-1486. doi:10.1016/j.cptl.2022.10.003
14. Janke KK, Bloom TJ, Boyce EG, et al. A pathway to professional identity formation: Report of the 2020-2021 AACP student affairs standing committee. American Journal of Pharmaceutical Education. 2021;85(10). doi:10.5688/ajpe8714
15. Luyckx K, Goossens L, Soenens B, Beyers W. Unpacking commitment and exploration: Preliminary validation of an integrative model of late adolescent identity formation. Journal of Adolescence. 2005;29(3):361-378. doi:10.1016/j.adolescence.2005.03.008
16. AFPC Educational Outcomes for First Professional Degree Programs in Pharmacy in Canada 2017. Association of Faculties of Pharmacy of Canada. Accessed August 26, 2023. http://www.afpc.info/system/files/public/AFPC-educational%20Outcomes%202017_final%20Jun2017.pdf
17. Elnicki DM. Learning with emotion: which emotions and learning what? Acad Med 2010;85:1111.
18. Poulsen L, Brosen K, Arendt-Nielsen L, et al. Codeine and morphine in extensive and poor metabolizers of sparteine:pharmacokinetics, analgesic effect and side effects. Eur J Clin Pharmacol. 1996. 51(3-4): 289-295.
19. Caraco Y, Sheller J, and Wood AJ. Pharmacogenetic determination of the effects of codeine and prediction of drug interactions. J Pharmacol Exp Ther. 1996. 278: 1165-1174.
20. Lalovic B, Phillips B, Resler LL, et al. Quantitative contribution of CYP2D6 & CYP3A4 to oxycodone metabolism in human liver and intestinal microsomes. Drug Metab Dispos. 2004. 32: 447-454.
21. Campfield KM, Hills AM. Effect of timing of critical incident stress debriefing (CISD) on posttraumatic symptoms. J Trauma Stress. 2001;14(2):327-340. doi:10.1023/A:1011117018705
22. Formative Assessment and Feedback. Stanford | Teaching Commons. Accessed August 16, 2023. https://teachingcommons.stanford.edu/teaching-guides/foundations-course-design/feedback-and-assessment/formative-assessment-and-feedback#:~:text=Formative%20feedback%20helps%20students%20recognize,to%20meet%20the%20course%20outcomes.
23. Formative and Summative Feedback. Teaching@Tufts. Accessed August 6, 2023. https://sites.tufts.edu/teaching/assessment/assessment-approaches/formative-and-summative-feedback/.
24. Mann B. 3 of America's biggest pharmacy chains have been found liable for the opioid crisis. November 23, 2023. Accessed August 16, 2023. Ohio jury holds CVS, Walgreens and Walmart liable for opioid crisis : NPR
25. Wile R. CVS and Walgreens to pay a combined $10.7 billion settlement for alleged opioid prescription lapses. December 12, 2022. Accessed August 16, 2023. CVS, Walgreens to pay $10.7 billion for alleged opioid prescription lapses (nbcnews.com)