| The University of Connecticut School of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Statements of credit for the online activity ACPE UAN 0009-0000-23-056-H08-P/T will be awarded when the post test and evaluation have been completed and passed with a 70% or better. Your CE credits will be uploaded to your CPE monitor profile within 2 weeks of completion of the program. |
Content
INTRODUCTION
Dotty is an 84-year-old widow suffering from osteoarthritis of the knees. Most days, she manages her pain with acetaminophen and has remained active in her community. Some days however, her painful knees make her unsteady on her feet and she has come close to falling, especially during the long walk from the parking lot through the senior center to get to BINGO.
Managing chronic pain—pain lasting three months or more—in older community dwellers is a challenge due to the link between pain and increased risk of falls. Over-the-counter (OTC) and prescribed pain medication further compound fall risk through adverse effects. More than 100 million adults in the United States (U.S.) suffer from chronic pain.1 Common types of chronic pain include neuropathic, musculoskeletal, inflammatory, and mechanical pain. Between 30% and 40% of community-dwelling people older than 65 and 50% older than 80 fall each year.2
Despite the use of fall prevention programs, the rate of falls resulting in injury has not declined. Researchers conducted a pragmatic, cluster-randomized trial (N = 5451) at 86 primary care practices across 10 U.S. health care systems. The trial evaluated the effectiveness of a multifactorial intervention including fall risk assessment and individual fall reduction plans compared to a control group receiving usual care. The results of the study found intervention did not significantly lower fall rates.3
Many factors contribute to falls, but compelling evidence suggests that chronic musculoskeletal pain increases fall risk and people living with chronic pain show poorer executive function (mental skills that include working memory, flexible thinking, and self-control). Signs of poor executive function such as impaired impulse control, reduced ability to pay attention or focus, and problems starting, organizing or planning tasks can all contribute to fall risk. Treatment options for chronic pain include physical and behavioral medicine, neuromodulation, and surgical intervention. Despite a variety of treatment options, providers most frequently use pharmacologic approaches.
Integrated, patient-centric, multi-disciplinary management of chronic pain offers a practical solution to reducing pain, over-medication, and risk of falls. Practitioners from several disciplines can help:
- Pharmacists understand how medications work individually and in combination and provide medication management that is more informed than other professionals’ medication management.
- Pharmacists and pharmacy technicians interact routinely with the community and can provide risk screening, patient education, and referrals to other HCPs.
- Primary care physicians provide medication management including medication review and reconciliation and oversight for changes from multiple providers. Providers correctly prescribe but may not evaluate medications regularly for appropriateness.
- Physical therapists can reduce pain and improve functional mobility through exercise, modalities (i.e., ultrasound, electric stimulation, iontophoresis), manual techniques, and prescription and training on assistive and adaptive devices.
- Physical or occupational therapists may provide in-home safety evaluation and recommend modifications and equipment to reduce the risk of falls.
- Collaborative relationships between community rehabilitation therapists and local pharmacies can support patient decisions and pathways for obtaining needed devices and aids to reduce pain and fall risk.
THE CLINICAL PROBLEM
Scope of Chronic Pain and Fall Risk
Falls are the leading cause of death and injury in people 65 years of age and older. Pain often contributes to fall-risk. According to a recent Helsinki Aging Study, 61% of community-dwelling people 74 years and older reported they suffer from musculoskeletal pain that interferes with activities of daily living.4
Because pain contributes to falls that result in further painful injuries, a cyclical pattern occurs. More than 50% of older Americans report pain at multiple sites.5 The most prevalent painful conditions affecting older adults include arthritis, chronic disease complications (i.e., diabetes, cancer) and post-stroke pain).6
In Dotty’s case, her painfully arthritic knees prompted her to purchase a three-wheeled folding walker with a seat from an infomercial she saw on daytime television. Unfortunately, it folded while in use, collapsing to the ground along with Dotty. She ended up with a severely bruised and painful hip as a result of the fall.
While environmental accidents and age-related changes can contribute to falls, chronic pain with medication use is a significant fall risk factor. In addition to polypharmacy, studies have shown both opioid use and exposure to nonsteroidal anti-inflammatory drugs (NSAIDs) contribute to fall risk. A retrospective, observational, multicenter cohort study of registry data in Canada (N = 67,929) concluded that recent opioid use is associated with an increased risk of falls in older adults and an increased likelihood of death from fall-related injuries.7 A systematic review also found an increased risk of falls is probable when elderly individuals are exposed to NSAIDs.8
A pharmacologic approach to pain may be necessary when pain is significant, unremitting, and affects physical function or quality of life. However, health care professionals should not overlook the importance of nonpharmacologic pain management. Non-pharmacologic pain management and the reduction of falls is an important health topic for consideration by pharmacists and pharmacy technicians.9
Economic and Socioeconomic Burden of Pain Related Falls
Serious injuries from falls can lead to permanent injury, functional and cognitive decline, reduced quality of life and the need for institutional care resulting in significant cost.10 The American College of Rheumatology, a leading authority and partner of rheumatology professionals, considers pain chronic when it lasts more than three months, the normal time for tissue healing. Chronic pain is a major cause of disability and linked to mental health deterioration including depression and anxiety.11
Professionals use many evidence-based fall prevention programs, such as those listed on the National Council on Aging website (Evidence-Based Falls Prevention for Older Adults (ncoa.org) to reduce falls in the community. These interventions vary in length such as 2-hour workshops, in-home interviews, or 8 week to 5-month programs that focus on aging in place, exercise, balance, removal of home hazards, adaptive equipment, task modification, education, and self-management.
Even with fall prevention programs, the number of falls among older community dwellers is increasing. The reason for the rising number of elderly falls is multifaceted12,13:
- The population of older adults is growing with more people living longer and remaining in their homes.
- Access to and participation in fall prevention programs varies among community elderly.
- In an aging population, musculoskeletal disability and resulting pain increases.
- As musculoskeletal disability increases, the number of invasive joint surgeries such as hip and knee replacements rises. The projected volume of primary total knee replacements alone will increase by more than 400% over the next 20 years.
- 7% to 23% of patients after hip and 10% to 34% after knee replacement have long-term post-operative pain.
When surgeries such as joint replacement result in chronic pain, providers primarily use medication to address pain due to limited treatment options. The combination of aging, more joint replacement surgeries, and concomitant medication use requires more attention to pharmaceutical services in the role of fall prevention. Furthermore, age-related changes in pharmacokinetics and pharmacodynamics may increase the risk and incidence of adverse drug events related to falls.6
IMPACT OF PAIN MEDICATION ON FALLS
Risk of Opioid Use in the Elderly
After her fall, an ambulance whisked Dotty to the hospital. Luckily, she did not sustain any fractures and the emergency department physician sent her home with a prescription for opioids, advised follow up with her primary care doctor, and gave her a flyer for a local fall prevention program.
The use of opioids for pain management is a significant public health concern particularly among older community dwellers at risk for falls. Prescribed opioid use among middle-aged and older adults is more prevalent than among younger adults.14 Moreover, one-fourth (25.4%) of adults aged 65 years and older who take opioids report being long-time opioid users for a period of 90 days or longer (see Figure 1).15
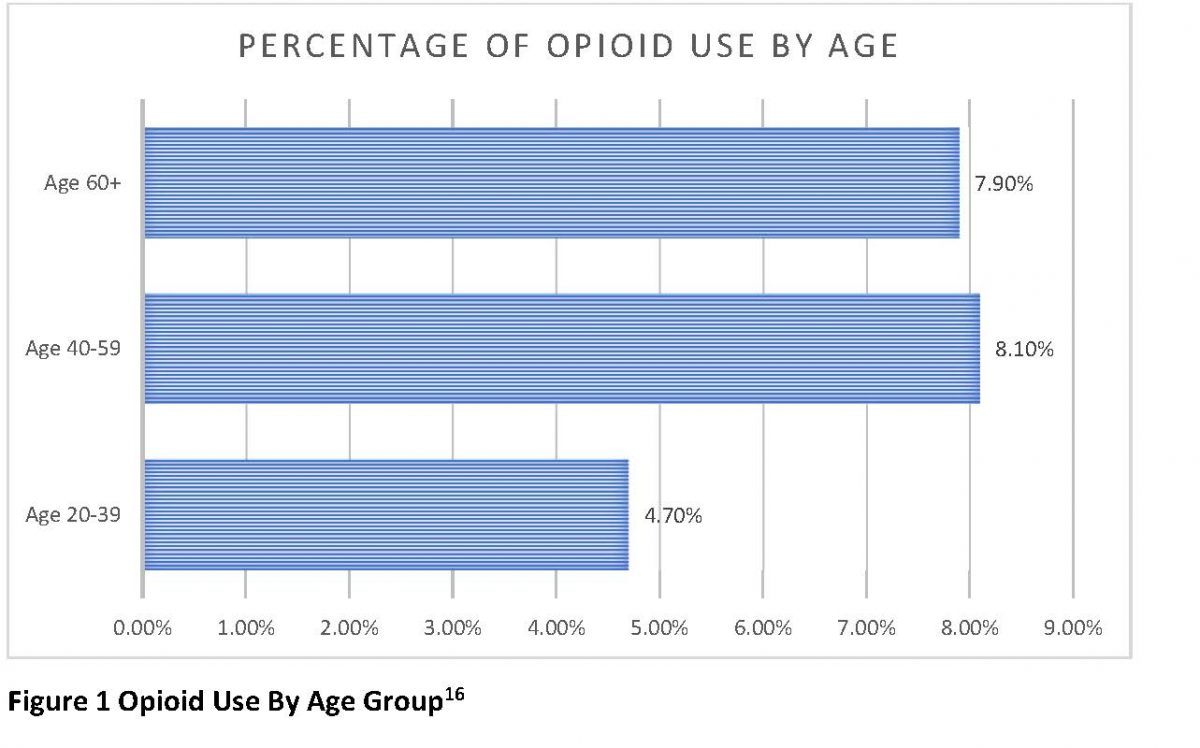
An average of 8.6 million non-institutionalized older adults filled at least one opioid prescription between 2018 and 2019, while 2.7 million older people filled five or more opioid prescriptions or refills. Older women were more likely than men to fill one or more opioid prescriptions.16 In addition to age, socioeconomic factors and patient demographics impact opioid use. According to the statistical brief published by the Agency for Healthcare Research and Quality (AHRQ), elderly adults who were poor filled five or more opioid prescriptions compared to low- and middle-income adults (see Figure 2).16

A large retrospective, observational, multicenter cohort study of registry data of 67,929 Canadian patients with a mean age of 80.9 (±8.0) evaluated the link between recent opioid use and fall-related injuries. The study identified patients who had filled an opioid prescription in the two weeks preceding an injury were 2.4 times more likely to have a fall than any other type of injury. Patients who had a fall-related injury who used opioids were also at increased risk of in-hospital death.7
A systematic review and meta-analysis of 30 studies evaluated the impact of opioid use on falls, fall injuries, and factures among adults at least 65 years old. The study found that opioid use was associated with falls, fall injuries, and fractures.17
Sedation is a common adverse effect of opioids. Medication with sedative effects can lead to daytime drowsiness, reduced alertness, and impaired motor function. Older adults experience these adverse effects more frequently, particularly during the first few days of taking a new pain medication.18 Anticholinergic burden is one of the opioids’, such as oxycodone, lesser-known effects. Anticholinergic drugs impact central nervous system functions and can result in cognitive impairment, confusion, and blurred vision compounding the risks of sedation.19
Because opioids cause drowsiness, orthostatic hypotension (dizziness or lightheadedness when standing up or otherwise changing position), and hyponatremia (low sodium levels leading to nausea, vomiting, loss of energy and confusion), they can increase fall risk. Risk is more prominent in older adults already prone to falls. Active drug half-life and metabolites are prolonged in older adults with renal impairment because most drugs, particularly water-soluble drugs, are eliminated by the kidneys.20 Understanding renal function is therefore important when assessing dosing risks in the older population. Reviewing for combination opioid use is also important in all patients, and particularly older patients. For example, physicians and pharmacists must take caution with patients using codeine and oxycodone together.21
Risk of OTC Pain Medication
Physicians often prescribe acetaminophen as a first-line or preferred OTC pain medication for older adults with nociceptive pain, which is pain caused by physical trauma, burns or surgery, because of potential adverse effects of NSAID (diclofenac, etodolac, fenoprofen, ibuprofen, ketorolac, meloxicam , naproxen) use. Long-term NSAID use is associated with adverse gastrointestinal, renal, and cardiovascular effects. An observed decrease in prescription NSAID and acetaminophen use may be due in part to the increased availability and variety of OTC NSAIDs over time, a phenomenon reported for other medications after becoming available OTC.22
NSAIDs are among the 5% to 10% most commonly prescribed medications for pain and inflammation. The prevalence of NSAID use in the over-65 population is as high as 96%.23 Physicians and other healthcare providers often prescribe NSAIDs for acute or chronic arthritic pain because of their anti-inflammatory results over just the analgesic effect of acetaminophen.22
Problems may arise related to NSAID-related toxicity in the elderly. Similar to opioids, age-related changes in pharmacokinetics may affect how the elderly metabolize NSAIDs. Dose reduction is appropriate for naproxen, ketoprofen, and salicylates in healthy older patients. Additionally, prescribers may need to reduce the dosage of diflunisal, indomethacin, sulindac, and mefenamic acid for the elderly in the presence of renal disease.24
Table 1 lists the adverse effects of long-term use of NSAIDs that can impact fall risk.
Table 1. NSAIDs Adverse Effects23
| System | Adverse Effects |
| Kidney | Increased risk of nephrotoxicity
Promotes renal vasoconstriction and reduced renal perfusion Electrolyte imbalance such as hyperkalemia Reduced glomerular filtration rate Nephrotic syndrome Chronic kidney disease Acute interstitial nephritis Sodium retention Edema Renal papillary necrosis |
| Gastrointestinal | Increased risk of GI bleeding |
| Cardiovascular | Edema
Myocardial infarction Thrombotic events Stroke Hypertension |
Study data has been inconsistent but overall trends support an association of falls with NSAIDs use in the elderly. A systematic review of 13 studies published between 1966 and 2008 specifically reviewed fall risk associated with NSAIDs in the elderly population. The overall mean age of study participants was high, preventing generalizability to a larger population. However, all studies showed an increased risk of falling associated with NSAIDs.8 A similar systematic review identified 22 studies that enrolled patients older than 60 years to assess the association between medication use and falling. These analysts reviewed nine different drug classes (antidepressants, antihypertensives, benzodiazepines, beta-blockers, diuretics, narcotics, neuroleptics and antipsychotics, NSAIDs, and sedatives and hypnotics) encompassing 79,081 participants. The use of sedatives and hypnotics, neuroleptics and antipsychotics, antidepressants, benzodiazepines and NSAIDS resulted in an increased likelihood of falling. The unadjusted odds ratio estimate for likelihood of falls related to NSAIDs was 1.21 (95% CI, 1.01-1.44) compared to 0.96 (95%CI, 0.78-1.18) for narcotics.25
The Case for Non-Pharmacologic Pain Management
The evidence supporting the need for nonpharmacologic pain management treatment is compelling. The population is aging, the prevalence and incidence of musculoskeletal disability is on the rise, and use of pain medication is associated with known risks. While all adverse effects of taking pain medication are important, falls can be among the most debilitating and costly for the elderly.
Pharmacists and pharmacy technicians are front line community healthcare providers in pivotal positions to positively impact fall reduction. By moving beyond medication management, pharmacists and pharmacy technicians can proactively participate in a multi-disciplinary approach to reduce reliance on pain medication and facilitate non-pharmacologic treatment including physical therapy.
DEVELOPING AN INTEGRATED PATIENT-CENTRIC TEAM-BASED APPROACH TO FALL PREVENTION
Pharmacists’ Role in Medication Management
Pharmacists play a key role in fall prevention by recognizing “fall risk-increasing drugs” (FRIDs), identifying at-risk patients, and collaborating with other healthcare professionals including physicians, home care nurses, and physical therapists by making appropriate referrals.
A traditional first step for pharmacists and pharmacy technicians is medication management. Knowing FRIDs is important (see Table 2).
Table 2. FRIDs at-a-glance
| Classes of Fall Risk-Increasing Drug | |||
| Antidepressants | Antihypertensives | Opioids | NSAIDs |
| Anticonvulsants | Antipsychotics | Sedative hypnotics | Antispasmodics |
| Anticholinergics | Benzodiazepines | Antihistamines | Antispastics |
Polypharmacy, exposure to FRIDs, or the combination of polypharmacy including FRIDs can be associated with fall risk. Pharmacists should also consider exposure to potentially inappropriate medications (PIMs) as described in prescribing guidance tools such as the American Geriatric Society (AGS) Beers Criteria.26
The Beers Criteria considers five broad categories of potentially inappropriate medications used in the elderly27:
- Medications considered potentially inappropriate
- Medications potentially inappropriate in patients with certain diseases or syndromes
- Medications to be used with caution
- Potentially inappropriate drug-drug interactions
- Medications whose dosages should be adjusted based on renal function.
Additionally, the National Council on Aging (NCOA) advocates for a thorough medication review for older adults at risk of falling, noting that OTC medications can cause harmful interactions and increase falls.
The five important problem areas identified by pharmacists in conjunction with the program’s algorithms include28
- Unnecessary therapeutic duplication
- Use of medications that can cause falls and confusion
- Use of medications that can cause cardiovascular problems
- Inappropriate use of non-steroidal anti-inflammatory drugs
- Review for effectiveness of opioid prescriptions and alternate options
An example of unnecessary therapeutic duplication occurs when patients take a muscle relaxer such as meloxicam with an OTC for inflammation like naproxen. Many patients are also unaware of medications that can cause falls and confusion such as OTC antihistamines. Patient education directly from pharmacists or pharmacy technicians can be beneficial in preventing falls related to these types of OTC drugs.
After her fall, Dotty filled her opioid prescription and continued taking acetaminophen due to the pain in her knees and hip from the fall. Since her providers or pharmacist had not “prescribed” acetaminophen, they were unaware of the unnecessary analgesic duplication.
While medication management and identification of FRIDs is important to reducing risk of falls, it is not a substitute for a comprehensive multi-disciplinary approach. A recently published systematic review of the use of fall risk-increasing drugs looked at 14 observational or intervention studies that assessed FRID use in participants 60 years or older. Participants had experienced a fall resulting in a hospitalization or emergency department (ED) visit. The studies reported the prevalence of FRID use was 65% to 93% at the time of hospitalization or ED admission among older adults with a fall-related injury. Further, studies within the review found FRID use did not decrease at one and six months following a fall. Intervention trials included in the review demonstrated that interventions to reduce FRIDs did not result in a significant reduction in falls. The authors conclude that medication review with suggestions to the primary care provider as a stand-alone intervention was ineffective in preventing falls. Interventions to reduce FRID use are only one part of a more comprehensive strategy.29
Dosing and Deprescribing to Reduce Falls
When making decisions to deprescribe opioids, prescribers and pharmacists should consider whether the opioid use matches an appropriate indication. Since opioids are strong analgesics, their indications should be for moderate to severe acute pain, post-operative pain, or palliative care. Prescribers and pharmacists should always consider deprescribing when there are no indications for prescribing an opioid and safer alternatives are available.6
Opioid dosing should always be specific to the individual with lower doses for older adults. Reducing the dose or switching to a less potent analgesic to maintain effective pain management is a viable strategy while implementing other nonpharmacologic techniques such as physical therapy.6
Pharmacists are skilled in identifying medications for discontinuation based on known risks. A careful plan for tapering and discontinuing drugs at an appropriate pace is critical to avoid increasing patients’ pain, stress, and discouragement. Various tools are available to pharmacists to collaborate with patients to create a deprescribing plan.30 Examples of resources to assist healthcare providers optimize medications while minimizing adverse events include the Medication Appropriateness Index Calculator ( https://globalrph.com/medcalcs/medication-appropriateness-index-calculator/) and the AGS Beers Criteria available from the American Geriatrics Society (https://agsjournals.onlinelibrary.wiley.com/doi/full/10.1111/jgs.18372). No one tool is the gold standard and inconsistencies exist among the various resources.31
For example, the STOPPFall tool provides deprescribing in a stepwise manner.18 STOPPFall recommends reducing the opioid dose by 5% to 25% of the daily dose every one to four weeks. If adverse effects occur during deprescribing, prescribers can reduce the dose more slowly. If the patient dose is high or he or she has been using the opioid for a longer period, deprescribing should proceed very slowly.
Conversely another tool, MedStopper, indicates when a patient has been taking an opioid daily for more than four weeks, prescribers should reduce the dose by 25% every three to four days. Upon any symptoms of withdrawal, they should increase the dose back to 75% of the previous tolerated dose. Once at 25% of the original dose with no withdrawal symptoms, they can discontinue the drug.32 Prescribers and pharmacists should monitor patients during and after deprescribing for symptoms of withdrawal such as musculoskeletal or gastrointestinal symptoms, restlessness, anxiety, insomnia, diaphoresis (excessive sweating), anger, and chills.
Pharmacy Fall Risk Prevention Service
To be an integral part of a more comprehensive fall prevention intervention, pharmacies should consider offering a fall prevention service. Establishing a community fall prevention service consists of fall risk screening, consultation to assess modifiable fall risk factors with referral to appropriate non-pharmacological intervention, medication check, and comprehensive medication review and adjustment by the pharmacy and primary prescriber.
Use of an appropriate screening tool by pharmacists or pharmacy technicians is a major step to reducing risk of falls. To assist healthcare professionals in reducing fall risk, the Centers for Disease Control and Prevention (CDC) developed the STEADI (Stopping Elderly Accidents, Deaths, and Injuries) initiative. This initiative includes three steps for providers to address their patient’s fall risk.31,33
- Screening for fall risk by asking patients if they have experienced past falls, feel unsteady, or are afraid of falling
- Reviewing and managing their medications to determine if they impact fall risk and stopping, switching, or reducing them
- Studies shows recommending vitamin D supplements to improve bone, muscle, and nerve can reduce risk of falls in the elderly
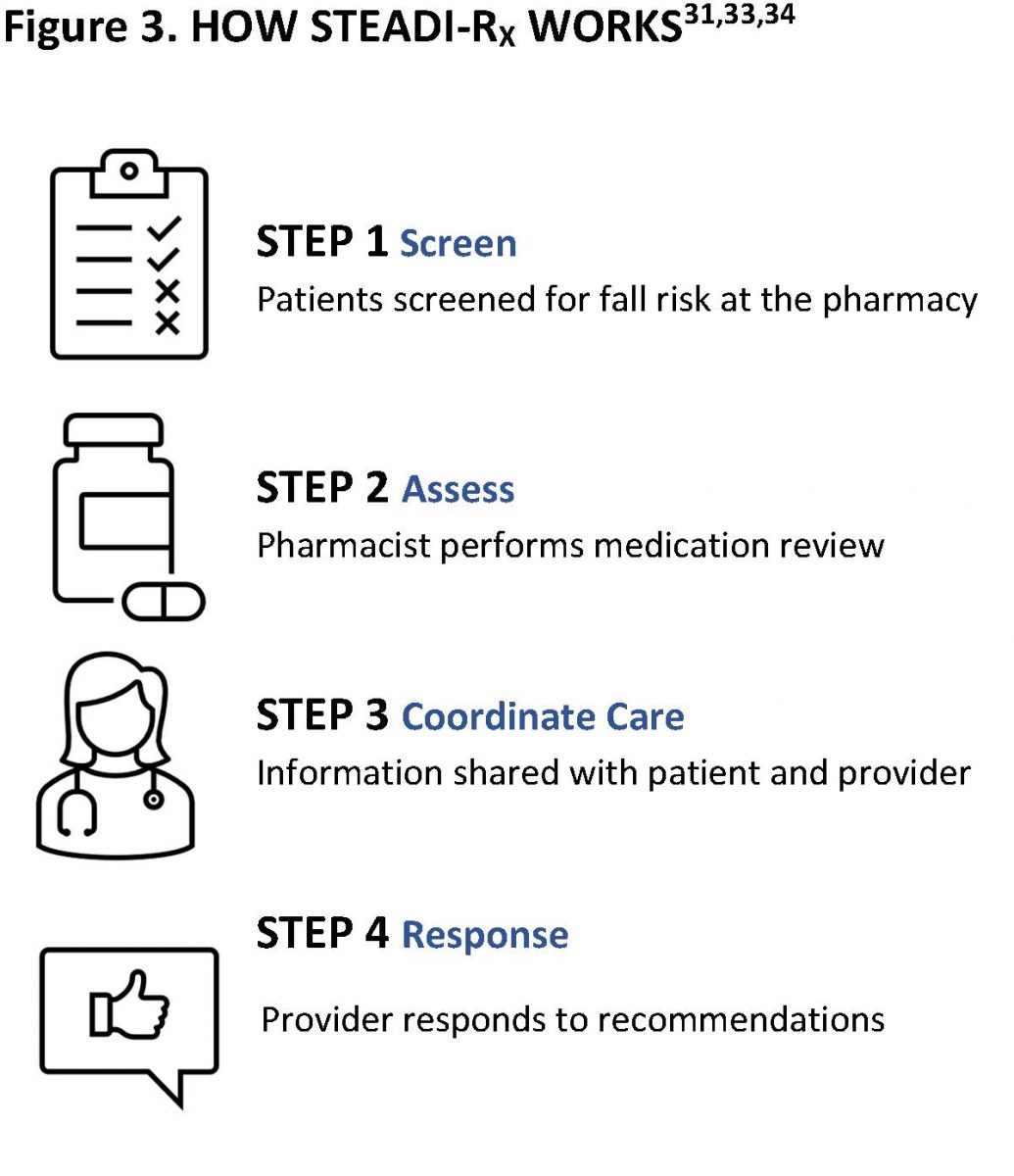
The CDC and the University of North Carolina Eshelman School of Pharmacy and School of Medicine developed an algorithm called STEADI-RX to improve collaboration between healthcare providers and pharmacists based on the CDC’s STEADI initiative. STEADI-RX incorporates the Joint Commission of Pharmacy Practitioners (JCPP) Pharmacists’ Patient Care Process and an algorithm for integrating fall screening and prevention into pharmaceutical care. It also includes a tool kit for use by healthcare providers to help reduce risk of falls.34 Figure 3 shows the STEADI-Rx’s key steps.
The STEADI-RX Community Fall Risk Checklist35 (https://www.cdc.gov/steadi/pdf/provider/steadi-rx/STEADIRx_pharmacy_fallrisk_checklist-508.pdf) is available to help the pharmacy staff quickly identify risk factors including fall history, postural hypotension episodes, and review medication classes associated with fall risk.
Getting Started with A Fall Risk Service
The STEADI-Rx Older Adult Fall Prevention Guide for Community Pharmacists, available from the CDC at https://www.cdc.gov/steadi/steadi-rx.html,36 provides a framework for how to start a fall prevention service, identifies best practices, and provides tools and references for implementing a successful program.
To start an in-pharmacy fall reduction program, a key recommendation is to first identify a program champion. This is either a pharmacist or trained pharmacy technician who will serve as the lead role and ensure proper design and implementation of the program. Next, an environmental scan may help identify the patient population that will benefit from the service and how it fits into existing workflow. A fundamental aspect of conducting an environmental scan may include an analysis of strengths, weaknesses, opportunities, and threats (SWOT) to identify any internal or external obstacles to implementation, described in Sample Fall Prevention SWOT Analysis.
SIDEBAR: SAMPLE FALL PREVENTION SERVICE SWOT ANALYSIS
STRENGTHS - Internal factors include available resources and staff
WEAKNESSES - Internal obstacles may be poor workflow or documentation procedures
OPPORTUNITIES - External factors to support a successful service include an age-appropriate population, supportive providers, and state physical therapy direct access provisions to facilitate referrals
THREATS - External factors that may hinder a successful service such as nearby pharmacies with strong prevention services, reimbursement or other financial factors inhibiting patient participation
The guide also recommends conducting a readiness assessment to determine the steps needed to implement the service and to develop an action plan. The readiness assessment addresses staffing, resources, and training needed and assure there is appropriate support from leadership before moving forward. Depending upon existing pharmacy workflow, a pharmacy technician can lead a fall prevention service with pharmacist support when they need clinical judgement and expertise.
Coordinating Care: Physical Therapy and Physician Support
Dotty eventually came into the pharmacy looking for a “better” assistive device. She seemed confused about what device to choose and reported she recently had a fall. With her permission, a fall risk screening revealed she was taking both NSAIDs and opioids and had not been referred to physical therapy. She stated the ED gave her a flyer for a fall prevention program, but she didn’t go because it conflicted with BINGO at the senior center.
Pharmacists and prescribers should consider practice guideline recommendations to determine when to make referrals to physical therapy for the nonpharmacologic treatment of pain. It is important to consider reducing reliance on opioids and inappropriate use of NSAIDs.
Data from the National Ambulatory Medical Care Survey identified 11,994 visits representing a cross-section of all age patients between 2007-2015 where ICD-9 (diagnosis) codes indicated new chronic musculoskeletal pain. The survey found that healthcare providers prescribed patients opioids 21.5% of the time when they presented with new symptoms of chronic musculoskeletal pain but prescribed physical therapy just 10% of the time.37
Numerous studies have examined the relationship between early physical therapy and opioid use for chronic musculoskeletal pain including back neck, shoulder, and knee. Due to its incidence, prevalence and associated costs, a preponderance of studies focused on low back pain (LBP). A retrospective analysis using commercial health insurance claims data from 2009-2013 observed 148,866 patients aged 18 to 64 years with a new primary diagnosis of LBP over a 1-year period. Compared to patients who received late or no physical therapy, patients who saw a PT first had an 89.4% lower probability of obtaining an opioid prescription.38
Another cross-sectional observational study using the National Ambulatory and National Hospital Ambulatory Medical Care Surveys between 1997 and 2010 also identified lower PT referral rates among LBP patients aged 16 to 90 years old insured by Medicare and Medicaid. The study estimated 170 million visits for LBP led to 17.1 million PT visits. Further, visits not associated with PT referrals were more likely to be associated with opioid prescriptions.39
Healthcare providers do not always prescribe nor do patients use physical therapy as a frontline treatment for chronic pain. Patients may use physical therapy along with other nonpharmacologic treatments, such as behavior health interventions or medication. Physical therapy is an integral part of multidisciplinary care, particularly to support success with opioid taper or cessation. Physical therapy treatments to reduce pain include exercise, manual therapy, electrical nerve stimulation, and other physical agents.
When conducting a pharmacy fall risk service, pharmacy staff may encounter patients with chronic pain who have not received physical therapy prior to treatment with pain medication. The screening process will be the first step in assessing true risk.
Pharmacy staff can use the STEADI-RX Provider Consult Form(s) for Medication or Fall Screening to share medication therapy problems with the patient’s provider or to refer the patient to a physical therapist for a full fall risk assessment.40,41 A physical therapist’s formal fall risk assessment is more in-depth than the screening tool used at the pharmacy and includes an evaluation of gait, balance, and strength. When using these forms or any other type of communication, states have different physical therapy direct access provisions and limitations. Pharmacies can verify the levels of patient access to physical therapist services in the U.S. through the American Physical Therapy Association (https://www.apta.org/contentassets/4daf765978464a948505c2f115c90f55/direct-access-by-state-map.pdf). After referral, physical therapists should respond within seven days. If they don’t, the patients or pharmacy should contact the PT again.
Pharmacists and pharmacy technicians identifying at-risk patients during an initial fall risk screening performed at the pharmacy should refer patients to physical therapy for a full fall risk assessment. Physical therapists use a variety of objective assessment tools to address gait and balance such as the Tinetti Balance and Gait Assessment, Berg Balance Scale, or Timed Up and Go test to determine fall risk and areas for intervention. Therefore, when implementing a pharmacy fall reduction service, it is important for pharmacists to develop relationships with local outpatient physical therapy clinics able to accept referrals for fall risk evaluations.
Because musculoskeletal pain is highly prevalent and a leading cause of disability, physical therapists are crucial members of the interdisciplinary pain management team. Physical therapists work effectively by providing nonpharmacologic treatment of pain incorporating various pain-relieving modalities such as transcutaneous electrical stimulation, heat or cold therapy, joint or soft tissue mobilizations or the use of braces or splints. In addition to physical therapy treatment to address pain, physical therapists also recommend various assistive and adaptive devices. Patients may use these devices to reduce pain through off-loading a painful limb or making mobility including ambulation and transfers (i.e., moving from one position to another such as from sitting to standing, or getting in or out of bed) easier and safer.
Improperly selected or poorly fitted devices can result in further injury, pain or falls. Receiving instructions and training on proper use of assistive devices and compliance with instructions has not been strongly correlated. A small (N=17) observational cross-sectional study and focus group investigated older adults’ use of walkers in the home setting compared to current guidance in an attempt to identify circumstances leading to deviation from instructions for use. This study observed incorrect use of walkers 16% to 29% of the time associated with reduced stability.42 Another study found comparable results from a questionnaire of 94 patients using a cane for hip pathology.;47% of these patients were using the aid in the incorrect hand and of this group, 64% used their dominant hand. Furthermore, 66% of respondents reported they never received instruction on the correct hand to use. The study concluded that a significant percentage of patients are using canes incorrectly which may be due to lack of education.43
A patient-appropriate assistive device, when fitted and used correctly, can reduce pain and increase physical activity in patients with chronic pain, painful or impaired gait and other mobility issues. Selection and fitting of an assistive device should always be conducted through a PT evaluation. PTs use a multi-factorial assessment of the patient’s physical and cognitive abilities of and consider the environment in which the patient will use the device (see 5 Factors of Device Prescription). PTs will also ensure devices match a patient’s height, weight, and size when selecting the best assistive device.
SIDEBAR: 5 FACTORS OF DEVICE PRESCRIPTION
- Cognitive Function
- Coordination
- Upper-body, hand and grip strength
- Physical endurance
- Walking environment
Upon competition of their evaluation, it is important for the therapists to know what types of OTC assistive and adaptive devices are available for purchase at local pharmacies to support patient needs. Although assistive devices are often available at physical therapy clinics, a patient’s health insurance plan may not include reimbursement for devices. Often OTC devices and aids are priced lower at retail locations and purchased directly by patients or family members.
Rather than have Dotty guess and purchase a “better” assistive device, the pharmacy referred her to a physical therapist who determined that at least initially, a 4-point walker with front wheels would provide her the most stability and allow her to walk safely in both her home and the community.
Table 3 describes items often recommended by therapists to reduce pain, fall risk, and improve home safety. See Fun Facts to learn about the history of walkers.
Table 3. Assistive & Adaptive Devices
| Item | Description | Purpose |
| Bed Rails | Railing inserted between mattress and box spring or physically attached to bedframe | Assist with transfer out of bed by allowing people to pull their body to change position using arms/upper body |
| Cane, Walker | Ambulation assist devices. Canes can be single point, multi point (quad) and walkers with or without wheels | Provides additional point of contact to improve balance, alleviate weakness, or offload a painful joint |
| Commode, Raised Toilet Seat, Toilet Seat Rails | Portable toilet, elevated seat or arm rails | Assist with safe transfer on and off toilet |
| Grab Bars | Bars and railings permanently affixed to walls near showers, toilets, entry ways, steps, stairs | Promotes safe transfers from sit to stand, up and down stairs, in and out of shower |
| Grabbers or Reachers | Reaching aid with grab assist | Allows items to be safely grabbed if out of reach or if mobility, pain, or strength impairs reaching and grabbing |
| Neoprene braces and wraps | Supportive and compressive wraps and braces for ankles, knees, wrists | Provide joint protection, stability, and pain relief |
| Shoe wedges or inserts | Partial or full inserts used inside of shoes | Cushion or improve postural alignment to offload painful foot |
| Shower Chairs | Waterproof, quick dry, slip resistant stool or chair | Allows safe seating in shower to reduce slipping or falling and fatigue with standing |
SIDEBAR: FUN FACTS43,44,45,46
A walker, walking frame, or rollator is a mobility device used by people suffering from leg or back pain, weakness, impaired balance, amputation, or poor stamina.
- Walkers first appeared in the 1950s.
- The first US Patent was awarded in 1953 to William Cribbes Robb of the United Kingdom for device called a “walking aid” filed with the British patent office in 1949.
- Two US patents in 1957 are for variants with wheels.
- The first non-wheeled designed walker was patented in 1965 by Elmer F. Ries of Ohio. In 1970, Alfred Smith of California patented the first walker resembling modern day walkers.
Establishing Effective Team Communications
Communication between pharmacists, prescribers, and therapists is important to monitor progress and avoid symptoms of medication withdrawal. As patients progress with their therapy plan of care, medication dosing may be easier to adjust. Ongoing patient education from pharmacists and pharmacy technicians can help avoid unnecessary patient self-medication with OTC pain relievers during the transition period.
The physician or primary care provider receives regular updates from the physical therapy team and can provide the pharmacy with necessary progress to help coordinate dose reduction or deprescribing. When designing the workflow for a pharmacy fall prevention service, the program champion should be sure to include a schedule for giving and receiving team updates.
With ongoing treatment, the physical therapist reported Dotty was making progress toward her therapy plan of care goals. Upon completion of therapy Dotty would be stronger, have less pain, and reduce or eliminate pain medication, and graduate to using a single point cane as needed. Since Dotty’s Medicare insurance plan only covered the cost of the 4-point wheeled walker, she would have to purchase the cane out-of-pocket and would be returning to the pharmacy with the PT’s recommendation so that the PT could fit and train Dotty on its proper use during her therapy sessions.
Closing the Treatment Gap
The benefits of a pharmacy fall reduction service are multi-fold. Moving beyond medication management closes the current treatment gap in the delivery of consistent and effective fall prevention. By working collaboratively with other HCPs, pharmacists help achieve better fall prevention outcomes by reducing or eliminating pain medications while facilitating non-pharmacologic pain management and improved functional mobility improvement.