| The University of Connecticut School of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Statements of credit for the online activity ACPE UAN 0009-0000-22-046-H01-P/T will be awarded when the post test and evaluation have been completed and passed with a 70% or better. Your CE credits will be uploaded to your CPE monitor profile within 2 weeks of completion of the program. |
Content
Introduction
Monkeypox is a rare virus believed to be transmitted to humans from animals and is endemic to Central and West Africa, typically near tropical rainforests.1 There are two clades (groups that share a common biological ancestor) of monkeypox virus: the West African clade and Congo Basin clade. More severe illness has been reported from the Congo Basin clade. Monkeypox is caused by monkeypox virus, a member of the Orthopoxvirus genus.2
The U.S. Centers for Disease Control and Prevention (CDC), in coordination with state and local officials, have initiated an emergency response to identify, monitor, and investigate monkeypox. This response includes a Health Alert Network (HAN), which is developing public health and clinical recommendations by developing protocols, medical guidance, and facilitating delivery of vaccine postexposure prophylaxis (PEP). The HAN also provides evolving education regarding antivirals that the U.S. government has stockpiled for preparedness and response purposes.2 Antivirals are discussed later in this continuing education activity.
Exposure to Monkeypox
Much like how we peel a banana to see what is underneath, let’s peel away the mystery of monkeypox exposure. Transmission of the monkeypox virus to humans can occur via animal bite or direct contact with the blood, meat, bodily fluids, cutaneous, or mucosal lesions of an infected animal. Human-to-human transmission by close direct contact and via exhaled large droplets is rare but can occur.3
Historically, human to-human transmission has been reported among household contacts and in other shared living quarters (e.g., in prisons). Transmission has also been reported in health care providers who have had close, sustained contact with a patient, objects, or materials that are likely to carry infection, such as bedding, clothes, utensils, and furniture. Touching and being face-to-face with someone who has symptoms are risk factors for exposure.2
Monkeypox can spread through close skin-to-skin contact during sex, including kissing, touching, and oral and penetrative sex with someone who has symptoms. Monkeypox rashes are sometimes found on genitals and in the mouth. Mouth-to-skin contact could cause transmission where skin or mouth lesions are present. It is currently unknown whether monkeypox can be spread through semen or vaginal fluids. People who have symptoms should avoid sexual contact with others. Until more is known, individuals should continue using condoms after they recover, and continue using condoms until we know more about this virus’s transmission.4
Although the evidence is limited and the risk of human-to-human transmission appears to be low, researchers report that infants and young children appear to be at the greatest risk of severe disease.5 The World Health Organization (WHO) reports that transmission from the mother to the fetus can occur via the placenta (which can lead to congenital monkeypox) or by close contact during and after birth.1
Symptom Presentation
Just like a variety of recipes include bananas, patients with monkeypox can experience a variety of symptoms. Patients with monkeypox typically experience a febrile prodrome five to 13 days after exposure (range = four to 17 days), which often includes lymphadenopathy (abnormal enlargement of the lymph nodes), malaise, headache, and muscle aches. The prodrome might vary depending on the nature of exposure. The onset of a characteristic skin rash generally occurs one to four days following the prodrome. The lesions are well defined and progress over time to scabs. The rash can be disseminated.2
The monkeypox rash progresses through sequential stages6:
- Macules—small spots, different in color from the surrounding tissue
- Papules—small circumscribed solid elevations on the skin
- Vesicles—small, circumscribed elevations on the skin containing fluid
- Pustules—small, circumscribed elevations of the skin containing purulent material
- Scabs—crust formed by coagulation of blood, pus, serum, or a combination
The rash can last up to a month.1 The rash can also be confused with other diseases that are more commonly encountered in clinical practice (e.g., secondary syphilis, herpes, and varicella zoster). Researchers report some patients are co-infected with monkeypox virus and other infectious agents (e.g., varicella zoster or syphilis). Patients with a characteristic rash should be advised to receive testing.2
Monkeypox’s clinical presentation is occasionally inconsistent. Some cases present classically, while other cases are atypical. Common symptoms include genital and peri-anal lesions, fever, swollen lymph nodes, and pain when swallowing. Oral sores remain a common feature in combination with fever and swollen lymph nodes. In some cases, pustules appear before classical symptoms (e.g., fever) and lesions appear at different stages. Anogenital rash (with vesicular, pustular, or ulcerated lesions) sometimes appears first without spreading to other parts of the body. This initial presentation of a genital or peri-anal rash suggests close physical contact as the likely route of transmission, such as during sexual contact.7
Pause and Ponder Question: How often should you ask patients with fever if they have also had close contact with someone with similar symptoms or a rash or headache?
Avoiding Monkeypox
Some learners may avoid eating bananas. Let’s avoid monkeypox. As of June 2022, clinicians in Europe, North America, South America, Africa, Asia, and Australia have reported monkeypox cases. Public health officials are cautioning travelers to avoid close contact with dead or live wild animals such as small rodents and monkeys. Travelers should avoid eating prepared meat from wild game or using products such as creams and lotions derived from wild animals in Africa, where cases of monkeypox are mainly found.8
Health care professionals should continue to watch for updates and evolving guidance as more information becomes known. The CDC raised its alert level for monkeypox to level 2. (see Figure 1) An example of evolving guidance is that, initially, the CDC recommended that people wear masks when traveling. A few days later, the advice regarding mask-wearing is no longer present on the CDC web sites. Thus, their advice evolved.2 Travel watch alert level 2 continues to encourage people to practice enhanced precaution measures, such as avoiding contact with visibly sick people and regularly washing hands.9
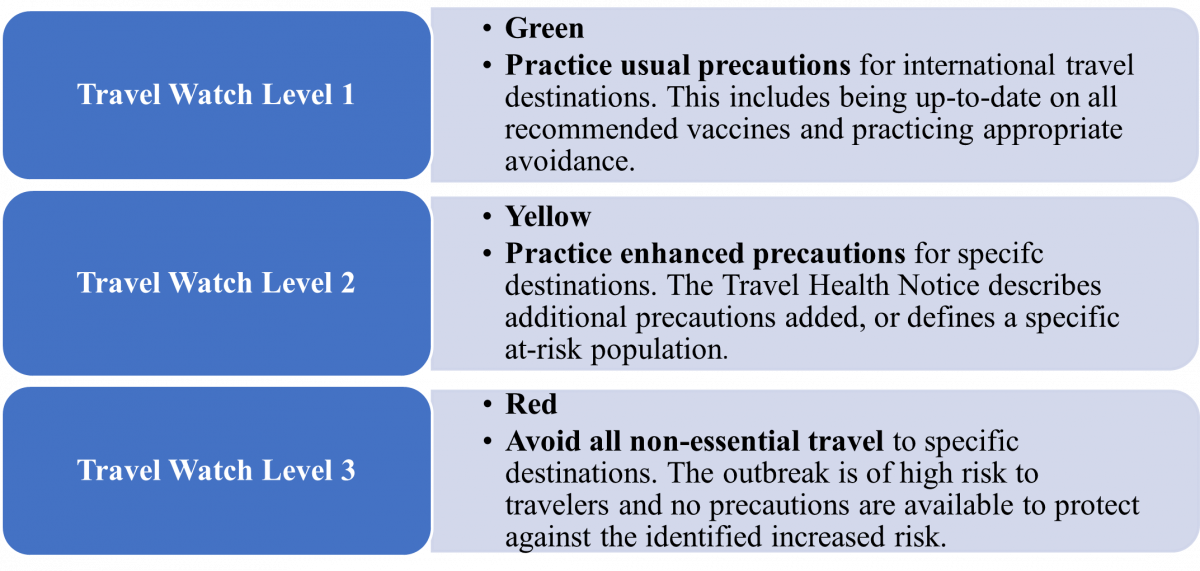
Figure 1. Centers for Disease Control and Prevention Travel Health Notices9
Researchers recommend the following measures to prevent infection with monkeypox2:
- Isolate ill people from uninfected people
- Practice good hand hygiene and use appropriate personal protective equipment to protect household members if ill or caring for ill persons at home (e.g., long sleeves and pants, and disposable gloves)
- Use an Environmental Protection Agency–registered disinfectant with emerging viral pathogens claim that is found on its List Q for disinfection of surfaces. Examples include hydrogen peroxide, isopropyl alcohol and citric acid among others.10 This list is available at https://www.epa.gov/pesticide-registration/disinfectants-emerging-viral-pathogens-evps-list-q
- Patients should also avoid contact with pets and other animals while infectious, because some mammals might be susceptible to monkeypox
- A person is considered infectious from the onset of illness until all lesions have crusted over, those crusts have separated, and a fresh layer of healthy skin has formed under the crust
Pause and Ponder Question: How can you make individuals in your practice setting more comfortable about the U.S. monkeypox outbreak?
Potential Health Impact
The WHO communicates that monkeypox is less contagious than smallpox and causes less severe illness. Monkeypox is usually a self-limiting condition with the symptoms lasting from two to four weeks.1
For individuals with monkeypox, isolation precautions should continue until all lesions have resolved, the scabs have fallen off, and a fresh layer of intact skin has formed. Patients who do not require hospitalization but remain potentially infectious should isolate at home. Clinicians should discontinue isolation only after consultation with the local or state health department.10
Beyond self-limiting cases, severe cases can occur and may lead to a range of medical complications.1 Conditions leading to hospitalization have included the need to provide adequate pain management and the need to treat secondary infections.7 Agencies are communicating monkeypox updates quickly, so many unknowns remain. Data reports of mortality are widely inconsistent so are not discussed in this manuscript.
Learners should refer to their states’ public health departments to determine if and how they should report suspected or confirmed monkeypox.
Pause and Ponder Question: The WHO is considering a name change for monkeypox. What do you believe would be a clinically accurate name?
APPROACH TO TREATMENT
Scientists say the risk of monkeypox becoming established in non-endemic countries is real. The WHO urges affected countries to make every effort to identify all cases and contacts to control this outbreak and prevent further spread. The FDA has approved a vaccine and has allowed expanded access for additional treatments for monkeypox, but these are in limited supply.11
The WHO is developing a coordination mechanism for the distribution of supplies based on public health need. The WHO does not recommend mass vaccination against monkeypox. In the few places where vaccines are available, they are being used to protect those who may be exposed, such as health workers and laboratory personnel.11
In general, some countries may consider post-exposure vaccination, ideally within four days of exposure, for higher-risk close contacts such as sexual partners, family members in the same household, and health workers.11 The CDC facilitates the availability of vaccine post-exposure prophylaxis (PEP) to contacts with high-risk exposures (e.g., unprotected contact with a patient’s skin or mucous membranes, lesion, or body fluids).10
PEP is not recommended for people with low or uncertain risk (e.g., health care providers entering a patient’s room without eye protection). Eligible intermediate- and high-risk contacts are offered PEP with2,12,13
- smallpox (vaccinia) vaccine, live (ACAM2000) or
- smallpox and monkeypox vaccine, live, nonreplicating (Jynneos) vaccines.
Researchers and regulatory authorities have not communicated whether optimal doses of expanded access investigational new drug (EA-IND) therapeutics for patients presenting with monkeypox will be consistently the same or different from doses for other indications. Clinicians should consult the full prescribing information for each therapeutic for comprehensive information, and pharmacy technicians should use the approved prescribing information to find information on storage conditions if necessary. Table 1 lists FDA-approved treatments for people presenting with monkeypox. It also describes therapeutics with EA-IND protocols for monkeypox or treatments undergoing further research.
Table 1. Approved and Investigational Therapeutics for Monkeypox12-17
| Generic Name (Brand Name; Manufacturer) | Current FDA approved indication |
| Smallpox (Vaccinia) Vaccine, Live (ACAM2000) | Vaccine indicated for active immunization against smallpox disease for persons determined to be at high risk for smallpox infection |
| Smallpox and Monkeypox Vaccine, Live, Non-replicating (Jynneos) | Vaccine indicated for prevention of smallpox and monkeypox disease in adults 18 years of age and older determined to be at high risk for smallpox or monkeypox infection |
| Tecovirimat (TPOXX)
|
Capsules and injection indicated for the treatment of human smallpox disease in adults and pediatric patients weighing ≥ 3 kg |
| Cidofovir (Vistide) | Infusion indicated for CMV retinitis in patients with acquired immunodeficiency syndrome |
| Brincidofovir (Tembexa) | Tablets and oral solution indicated for the treatment of human smallpox disease in adult and pediatric patients, including neonates |
| Vaccinia immune globulin (human) (Vigiv) | Intravenous immune globulin indicated for the treatment of complications due to vaccinia vaccination, including eczema vaccinatum, progressive vaccinia, severe generalized vaccinia, vaccinia infections in individuals who have skin conditions, aberrant infections induced by vaccinia virus |
Smallpox Vaccine
The smallpox live vaccine listed in Table 1 is licensed for immunization in people who are at least 18 years old and at high risk for smallpox infection. It is contraindicated in individuals with severe immunodeficiency. Select warnings include myocarditis, encephalitis, ocular vaccinia, infants younger than 12 months, and pregnancy. Common adverse events include injection site reactions, malaise, fatigue, fever and headache.12 It can be used in people exposed to monkeypox if it is used under an EA-IND protocol. The smallpox vaccine is not currently available to the general public. In the event of another outbreak of monkeypox in the U.S., CDC will establish guidelines explaining who should be vaccinated.18
Smallpox and Monkeypox Vaccine
The FDA has licensed smallpox and monkeypox vaccine to prevent infection with smallpox and monkeypox viruses. Anaphylactic reactions after dosing are possible. In smallpox vaccine-naïve healthy adults, the most common injection site reactions were pain, redness, swelling, induration, and itching. The most common systemic adverse reactions were muscle pain, headache, fatigue, nausea and chills.13
Data from Africa suggests that this vaccine is at least 85% effective in preventing monkeypox. Effectiveness against monkeypox was concluded from a clinical study on the immunogenicity and efficacy data from animal studies. Researchers believe that vaccination after a monkeypox exposure may help prevent the disease or make it less severe.18
Tecovirimat
The U.S. government stockpiles tecovirimat.18 Tecovirimat reduces the production and release of enveloped orthopoxvirus in vitro for seven monkeypox virus strains.19 Tecovirimat use for monkeypox is not FDA approved, but the CDC holds a non-research expanded access EA-IND protocol that allows its use for primary or early empiric treatment of monkeypox in adults and children of all ages. Clinical trials demonstrate the drug is safe with only minor side effects.18 The injection is contraindicated in severe renal impairment. Clinicians should monitor for hypoglycemic symptoms. Both the capsules and injection may cause headache.14
Cidofovir and Brincidofovir
Data is not available on the effectiveness of cidofovir or brincidofovir in treating human cases of monkeypox. Both have proven activity against poxviruses in in vitro and animal studies. It is unknown whether a person with severe monkeypox infection will benefit from treatment with either antiviral, although their use may be considered in such instances.18 The CDC holds an expanded access protocol for both products that allows use of stockpiled cidofovir for the treatment of orthopoxviruses (including monkeypox) in an outbreak. Brincidofovir may have a better safety profile than cidofovir. Serious renal toxicity or other adverse events have not been observed during treatment of cytomegalovirus infections with brincidofovir compared to treatment using cidofovir.18
Vaccinia Immune Globulin
Data is unavailable on the effectiveness of vaccinia immune globulin (VIG) in treatment of monkeypox virus infection. Use of this immune globulin is under an EA-IND. Proven benefit in the treatment of monkeypox is currently undetermined; however, healthcare providers may consider its use in severe cases. VIG can be considered for prophylactic use in an exposed person with severe immunodeficiency in T-cell function for which smallpox vaccination following exposure to monkeypox virus is contraindicated.18 A boxed warning indicates maltose in immune globulin products may give falsely high blood glucose levels in certain types of blood glucose testing systems. Additional warnings include renal dysfunction, thrombotic events, and infusion rate precautions. The most common adverse drug reactions are headache and nausea.
Pause and Ponder Question: What side effects have your patients reported after receiving a vaccine?
Ancillary Treatment Options, Supportive Care
Bananas are considered comfort food by many people. What comfort care can be recommended for patients suffering with monkeypox? Monkeypox can impact multiple systems and co-infections are possible. Soap and water, povidone-iodine, silver sulfadiazine and moist occlusive bandages promote healing at lesions sites. Adequate hydration and nutrition and protecting vulnerable anatomical sites such as the eyes and genitals are critical. Treatment for pain is recommended but specific analgesics have not been specified.20
Antipyretics can be used for fever. Antiemetics can be used for nausea. For ocular infection, topical application of trifluridine has been used to resolve symptoms and to attempt to prevent possible ocular scarring. Topical or oral antibiotics have also been used in combination either to treat bacterial infection or as prophylactic therapy. Bronchodilation, nebulizer, or suctioning is recommended if the respiratory tract is affected.20
CONCLUSION
Pharmacists are knowledgeable about many viruses and now are engaged in conversations involving monkeypox. The CDC urges health care providers in the United States to be alert for patients who have rash or illnesses consistent with monkeypox, regardless of a patient’s gender, sexual orientation, history of international travel, or specific risk factors for monkeypox. All health care providers should contact their local or state health department if they suspect a case of monkeypox.