
| The University of Connecticut School of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Statements of credit for the online activity ACPE UAN 0009-0000-25-070-H99-P/T will be awarded when the post test and evaluation have been completed and passed with a 70% or better. Your CE credits will be uploaded to your CPE monitor profile within 2 weeks of completion of the program. |
Content
INTRODUCTION
Humans’ overall health is derived in part from our diets and physical activity. Diet plays a significant role in cardiovascular disease, gastrointestinal diseases, hypertension, and obesity.1,2 In November 2018, The University of Connecticut hosted a conference in Florence, Italy, called “The Mediterranean Diet from an Italian Perspective.” Historians, scientists, and nutrition experts with diverse backgrounds who were primarily from Italy presented comprehensive information about the Mediterranean diet to U.S. pharmacists and dietitians. This continuing education activity reviews information covered in that conference and provides pharmacy teams with a better understanding of the term, “Mediterranean diet.” Educated and accessible health professionals can potentially minimize the incidence of diet-related diseases.
The human diet has changed with time. Humans started as hunter-gatherers (also called foragers by proponents of the currently popular Paleo diet), which entailed considerable physical activity coupled with a high protein, low carbohydrate diet.
Some subsets of the human population shifted to an agricultural lifestyle about 11,000 years ago; this is a relatively recent change if one considers that humans have roamed the earth for roughly 2 million years. The change tended to localize groups of people, galvanize population growth, and eventually, allow the development of urban centers. In the last two centuries, these changes supported and encouraged global industrialization and urbanization.3,4
Many researchers have blamed the current epidemic of certain diseases on the change from whole foods to a high carbohydrate, processed diet associated with industrialization. They also cite relationship between the industrial revolution and the availability of (and perception that we “need”) processed foods, artificial sweeteners, and preservatives. Most people’s diets are completely different from either the hunter-gatherer or agricultural diet consumed by people who farmed. The combination of today’s diet coupled with sedentary lifestyle has led to unforeseeable, clearly preventable health consequences.3,4 Anthropologists have always looked for links between food and diet, human biological and cultural evolution, and population health. In the last 50 years, medical researchers have joined them.
Hippocrates once said, “Let food be thy medicine and medicine be thy food.” Today, the Western diet is generally high in saturated fat and sucrose, and contains insufficient fiber. This diet increases the risk of obesity, asthma, diabetes, and inflammatory bowel disease.5 Our society has evolved from older and seemingly healthier diets to less healthy diets replete with processed foods.
This continuing education activity focuses on the Mediterranean diet and its potential to impact health. Researcher Ancel Keys coined the phrase “The Mediterranean diet” to describe a diet he observed near Naples, Italy in the 1950s. The term does not actually describe how people of the Mediterranean currently eat, and its definition is imprecise and somewhat fluid today. The Mediterranean diet is based on a different food pyramid (discussed below) than the traditional pyramid seen in Westernized countries. The activity will cover Ancel Keys and his discoveries from the Seven Country Study alongside his cholesterol hypothesis. The diet, which is rich in fiber and fermented food and drinks, like wines and cheeses, can improve health by nourishing our gut microbiome (the microorganisms that comprise our gut ecosystem and are necessary to digest food, synthesize vitamins, metabolize drugs, and detoxify carcinogens; see SIDEBAR, page 3).
SIDEBAR
What is the Human Microbiome?
The human microbiome is the composition of microbes in the human gastrointestinal tract, their genes, and the environment they occupy. In other words, the microbiome is a freestanding ecosystem in each individual’s gut. Of the trillions of microbes that live in or on our bodies, about 90% live within the gastrointestinal tract. The microbiota genome vastly outnumbers the human genome.
Humans are born with a set of DNA and are germ-free. But over time, different organisms from the outside environment or from foods we consume begin to change our intestinal composition. These elements tend to shape the microbiota all over the body, and the microbes on the skin vary widely from the microbes in the gut. Microbial diversity helps our body function correctly and no two areas on our bodies host the same bacterial composition.
Recently, researchers have discovered that the microbiome plays a much larger role in health than originally believed. From infancy to death, humans feed their gut microbiome continuously. Each body adapts constantly based on diet. Disruption of the microbiome through poor eating habits and antibiotic use can contribute to the progression of diseases like irritable bowel syndrome, obesity, and cardiovascular disorders. The typical American diet—a diet that often depends on processed or ultra- processed foods—has deteriorated the typical individual’s microbiome.
The Mediterranean diet contains fermented foods, such as wines and cheeses and an ample portion of fiber, that maintain and nourish the microbiome and promote overall health. The Mediterranean diet contributes to a diverse group of gastrointestinal microbes.12 It provides prebiotics and probiotics. Patients may ask about prebiotics and probiotics, which are available as over-the- counter supplements. It’s important to know the difference, and to know that a good diet can provide both naturally.
A strong microbiome aids in vitamin synthesis, immune system function, and xenobiotic (chemical compounds [drugs, pesticides, or carcinogens] that are foreign to a living organism) metabolism. It also fortifies the intestine’s impermeability. Some xenobiotics affect health negatively, but others, like supplements and antibiotics, have health benefits. Other functions include biosynthesis of neuro-active metabolites and neurotransmitters like GABA, dopamine, and acetylcholine.
Nourishing the gut microbiome helps strengthen our body’s anti-tumor response. However, the microbiome is unable to take part in these functions without microbial diversity. More than 20% of our microbiome variability is associated with diet, drugs or supplements consumed, and overall body composition.
| Prebiotics | Probiotics | |
| What’s the difference?
|
Substances that
come mainly from fiber to feed the beneficial gastrointestinal bacteria |
Live bacteria found
in food and/or supplements
|
| Why do we use them?
|
To bolster beneficial
bacteria that can be converted into products with anti- inflammatory properties |
To increase the
amount of beneficial bacteria in the gut
|
| What are some examples?
|
Legumes, beans,
peas, oats, bananas, berries, asparagus, garlic
|
Sauerkraut, kimchi,
fermented cheeses, fermented vegetables, Lactobacillus and Bifidobacterium |
Ancel Keys: Linking Health to Blood Cholesterol Ancel Keys (1904-2004) was an American scientist who spent much of his postgraduate career at the University of Minnesota. He studied diet’s influence on health with a particular interest in cholesterol and coronary heart disease. His contributions to understanding diet’s effects on cardiovascular disease made him an icon in cardiovascular nutrition.14 Keys’ interest in cholesterol peaked after World War II (WWII) when he noticed a significant increase in heart disease mortality with the evolution of the American diet.15 Diets are often based on beliefs or perceptions, and at that time, the American people believed that protein from animal sources was the key to a strong nation.
Dinner always included meat.16 Following WWII, the American diet increasingly included convenience foods—casseroles, Spam, and meatloaf, among other high-calorie or highly processed meals—that allowed men and women to work and still have the family-style dinner they desired with little effort.16
In the early 1950s, Keys traveled to Europe and observed
- Italy and Spain had remarkably low rates of heart disease
- In both Italy and Spain, the wealthy had high rates of cardiovascular disease, but the working class poor had almost no cardiovascular disease
- People in Mediterranean countries consumed a diet starkly different than that consumed in the United
Keys commented on the diet of working class families in the Naples, Italy area, writing “Homemade minestrone or vegetable soup, pasta of endless variety, freshly cooked, with tomato sauce, and a sprinkle of cheese, only occasionally enriched with some bits of meat, or served with a little local seafood, a hearty dish of beans (...) red wine and fresh fruit always.”17 He appropriately described the basis of the Mediterranean diet. After noting how American and Mediterranean diets diverged, Keys gathered anecdotal evidence and speculated that dietary habits explained the differences in cardiovascular disease rates be- tween countries. Keys presented his ideas at the 1955 World Health Organization (WHO) meeting, only to be laughed at by senior scientists in attendance.18
Seven Countries Study & Cholesterol Hypothesis Motivated to dig for answers, Keys began the first multi-country epidemiological study to look for a causal relationship between low-density lipoprotein (LDL) cholesterol and coronary heart disease in 1958. This five-year study enrolled nearly 12,000 men aged 40 to 59 in Finland, Greece, Italy, Japan, the Netherlands, the United States, and Yugoslavia.19
Keys’ findings, translated into his cholesterol hypothesis, were controversial. The original hypothesis of simply “good fats vs. bad fats” consumption in relation to serum cholesterol unexpectedly needed to include other factors. These factors included the influences of the food and drug industries; level of sugar consumption; and the varying lifestyles of different cultures around the world. This posed a further question: “Is there a diet that is universally healthy for all?” It should be noted that the studies Keys performed were observational, and lacked randomization and control groups. Therefore causation cannot be confirmed. Keys’ critics tended to point out that he “cherry picked” his data to produce the results he desired.
By 1975, Keys—eager to disseminate his findings—published cookbooks and coined the term “Mediterranean diet.” (Copies of his original cookbook, How to Eat Well and Stay Well the Mediterranean Way, are still available at a price of about $500.00.) With the newly popular Mediterranean diet notion came two different concepts of diet: empiric and normative.
- The empiric concept of diet is objective, simple, and factual (i.e. what people eat is considered their diet).
- The normative concept of diet is subjective and “what ought to be” (i.e. people should or should not eat certain ways.”
Keys’ dietary recommendations, according to his research, are based on the normative concept, and he wanted to make dietary change attractive.14 Keys hoped that adults who adopted a Mediterranean diet lifestyle could reduce their chronic disease burden. Some of the disease states Keys anticipated would be improved by the Mediterranean diet included cardiovascular disease, diabetes, hypertension, and kidney disease.20
The Mediterranean diet, as Key’s described, mainly consists of fresh fruits and vegetables, beans and legumes, whole grains, bread, and pasta, with small amounts of animal-based proteins consumed less frequently.
Food marks people’s cultural, religious, personal, and social class identity. Food production not only shapes landscapes and environments, but it also shapes our health. Consuming food is traditionally considered to be a social act, as it brings people together. In many cultures, food is symbolic. So, what do we learn from our food culture? It begins with a socialization process, starting at birth—first with family and friends, then in school and at work. Socialization influences what is “normal” to eat, the acquisition of food itself, and what is available, based on region.
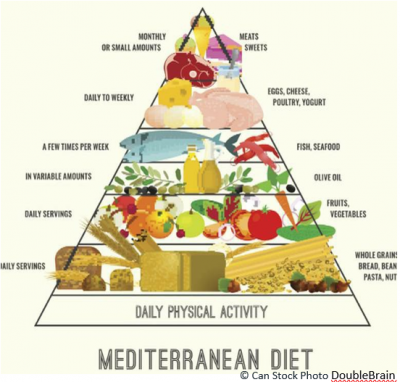
The Mediterranean Diet pyramid (Figure 1) varies significantly from most food pyramids. Starting at the figure’s base and working upward, conviviality (eating while enjoying good company) and physical activity are essential elements. Thus, the Mediterranean Diet is not only a diet, but a lifestyle. The diet is high in grains, legumes, and fresh produce consumed daily. Bread is served at most meals (see Sidebar on page 4), while meat is consumed less frequently. Olive oil, beans, nuts, legumes, seeds, herbs, and spices provide essential flavor to most meals. Fish or seafood is consumed at least twice weekly and wine is allowed in moderation (no more than five ounces of wine for women and ten ounces for men under the age of 65) daily.21
The Mediterranean diet is listed as a United Nations Educational, Scientific and Cultural Organization (UNESCO) Intangible Cultural Heritage of Humanity. An Intangible Cultural Heritage encompasses the oral traditions, performing arts, social practices, rituals, festive events, knowledge and practices concerning nature and the universe, or the knowledge and skills to produce traditional crafts.24 As described by UNESCO25: “The Mediterranean diet involves a set of skills, knowledge, rituals, symbols and traditions concerning crops, harvesting, fishing, animal husbandry, conservation, processing, cooking and particularly the sharing and consumption of food. Eating together is the foundation of the cultural identity and continuity of communities throughout the Mediterranean basin. It is a moment of social exchange and communication, an affirmation and renewal of family, group or community identity."
The diet’s intangible and cultural aspects make it unique; adherence to the diet is based on more than intake of specific foods. The conviviality and social aspect of eating together is an essential part of Mediterranean culture and is included as part of the food pyramid. Investigators have conducted trials to review how the Mediterranean diet affects health outcomes. The PREDIMED study conducted recently compared those who follow the Mediterranean diet to those who do not and their cardiovascular outcomes.
PAUSE AND PONDER: What does bread symbolize in your religion or culture?
Does it appear on the table at every meal?
SIDEBAR
BREAD
In the Mediterranean Diet, carbohydrates account for 45% to 55% of daily calories. This is because bread (among other grains) is the most important food in the Mediterranean and many other cultures; it is a symbol of sustenance and livelihood. Bread requires few ingredients, is inexpensive and easy to make, and provides nourishment. Each region of the world has its own way of making bread, from differences in ingredients to the techniques involved in the bread-making process itself.
The history of bread dates to the Ancient Egyptians in 8000 BC when they invented the first grinding stone, called a quern. The earliest breads more closely resembled porridge or a flat cake. Between 5000 and 3700 BC, bread became a staple food in Egypt and was also used for trade and bartering. Trading bread introduced it to other regions and cultures, expanding its production around the world. Over time, different types of grains and bread-making techniques emerged.
Greeks, Mexicans, Persians, and many others jumped on the bread bandwagon in the next several centuries. Each population created something unique. By 1000 BC, yeasted breads had become popular in Rome. Bread has always been a form of sustenance; for many centuries the type of bread one ate also represented status. Bread quickly became a symbol of Roman status. White breads were more expensive, and exclusively for the wealthy, while common people generally consumed darker whole wheat breads. The British adopted this same societal structure during medieval times.23
In many cultures “breaking bread” means bringing family and friends together for just a small meal or even a big holiday celebration.
In the Italian culture bread is revered for its symbolization of love and nurturing. Bread is never discarded but rather turned into an additional dish or crumbled in soup (ribollita). Consider the Italian tradition of sweeping breadcrumbs from the table into your fist and kissing them; it’s a symbol of the bread’s cultural importance.
Source: Reference 23
The PREDIMED Trial
Published by the New England Journal of Medicine in 2013 and again with corrections in 2018, the PREDIMED study assessed the Mediterranean diet in Spain from 2003 to 2011 and included 7447 men and women at high cardiovascular disease risk with a mean age of 67 years.26,27 The study was a multicenter, randomized, nutrition-intervention, primary prevention trial to test the efficacy of the Mediterranean Diet on the composite endpoint of death from cardiovascular cause, stroke and myocardial infarction. The researchers randomized subjects to one of three groups:
- Mediterranean diet supplemented with one liter per family per week of extra virgin olive oil
- Mediterranean diet supplemented with mixed nuts (1 oz/day) or
- A standard low fat control diet
While the intervention was originally intended to last six years, the researchers discontinued the trial early and advised all participants to follow a Mediterranean diet. The recommendation came after the study’s data and safety monitoring board realized that participants in either Mediterranean diet arm had significantly improved health statuses. After an average follow up of about 4.8 years, both Mediterranean Diet groups had a significant (30%) reduction in major cardiovascular events compared to the low fat control diet.27
However, after the 2013 publication, researchers raised questions about the study’s randomization and data analysis, indicating that errors in randomization introduced unintentional bias that made the results/data unreliable. The New England Journal of Medicine retracted the trial.26,28 The specific issue related to randomization was this: Randomization was not conducted consistently and correctly across all sites. For example, at some sites, if more than one participant per house enrolled, investigators would assign both individuals to the same diet. At other sites the research staff randomized entire clinics to a single treatment group instead of each participant.26,28
The authors reanalyzed and statistically corrected for correlations within families or clinics. The authors also reanalyzed the data and omitted 1588 participants whose trial group assignments were known or suspected to have deviated from the randomization protocol. After reanalysis of he remaining 5859 subjects, the authors found no significant changes from the original study. Reanalysis confirmed a 30% relative difference in major cardiovascular events in those randomized to the Mediterranean diet groups.26
Despite the controversy over the PREDIMED study, many studies have confirmed the Mediterranean diet’s benefits.29-31 The best time to internalize the elements of good diet is early in life, and in Italy, school systems follow and reinforce the Mediterranean diet’s general principles in their school lunch programs.
The program used in Florence, Italy is a good example.
PAUSE AND PONDER: How does the Mediterranean diet differ from what is perceived to be a healthy diet in the US? What factors other than food may play a role in its supposed health benefits?

School Lunch Program in Florence, Italy
While many children may learn the practices of the Mediterranean diet at home, the ideals of the normative Mediterranean diet are further ingrained in school through Italian school lunch programs. In the city of Florence, Italy, school staff prepares 24,000 lunches daily in 16 different kitchens. They deliver the meals to different primary schools. Menus rotate every four weeks and the menu changes three times annually to provide seasonally fresh foods. Pediatricians and dietitians develop the menu. Dietitians calculate protein, carbohydrates, fat, and calories for each meal to ensure that they are at national average. However, parents, chefs, and children have significant input as well. Parents are welcome to eat lunch with their children to try a school lunch. Dietary staff rarely serves canned or frozen food with the exception of peas and spinach in the winter. Menus indicate whether the food is organic, local, or both and about 90% of the food falls into these categories.32
Food from home is generally not allowed, and the school has no vending machines so all food originates from the kitchen. Fresh fruit is provided at around 10 AM in the classroom as a snack. Teachers eat with students during lunch. The lunch room accommodates about 20 students; children set tables, serve, or clear plates. At the end of each month, parents pay for their child’s lunch. The cost is income-based. The highest income level pays 4.90 Euros ($5.60 as of December 2018) per meal, and the lowest income level pays 1.00 Euro ($1.14 as of December 2018) per meal. Certain low-income groups do not pay.32 The main point is that Italy makes a healthy diet affordable for everyone, not just the wealthy.
Special meals are available to accommodate people who have a variety of food allergies. (Approximately 6% to 8% of the Italian population has allergies, yet roughly 20% of American children suffer from allergies.33 ) There are also Kosher, Halal, and vegetarian options. While chefs prepare these meals differently, they appear visually similar so students do not feel uncomfortable if they receive a different meal.32
Once children leave primary school, they no longer receive meals in school and it is up to the students and their parents to select foods they eat. The Mediterranean diet is instilled in the everyday lives of children who live in Florence through the school lunch program and these ideals many times continue into adulthood.32 If children continue these habits, evidence suggests health outcomes of interest to pharmacists and other healthcare providers (better cardiovascular health and less chronic illness).
Aging, Adherence to the Mediterranean Diet, and the Microbiome
Recently, researchers conducted a study to understand how adherence to the Mediterranean diet in an aging population can be a simple way for people to reduce cardiovascular risk.34 In a study of 476 adults aged 50 to 89 living in Italy, these researchers looked for a link between adherence to the Mediterranean Diet, cardiometabolic disorders and polypharmacy (defined as five or more medications). Using patient self-report, they found that patients who had medium-low adherence to the Mediterranean diet over the years took an average of five medications. Participants in the medium-low adherence group also had a higher body mass index, and a higher prevalence of arterial hypertension, previous coronary and cerebrovascular events, diabetes, and dyslipidemia on average compared to those in the high adherence group.
Those whose diet most closely resembled the ideal Mediterranean diet, however, took an average of three medications.
Their conclusion was that adherence to the Mediterranean Diet may decrease polypharmacy and cardiometabolic disorders in elderly, and have a positive preventive effects on health deterioration.34 Using the results of this study, pharmacists can explain to patients how diet changes can potentially affect their pill burden. Polypharmacy can lead to issues such as side effects and drug interactions that can be avoided with simple dietary changes. Dietary changes can also eventually lead to beneficial changes to the human microbiome.
The industrial revolution changed the American diet. Greater accessibility to a wide variety of foods and mass produced, convenient meals lead to microbiome degradation and dysfunction.35 Most of the food in American grocery stores does not nourish the microbiota, lacking the component key to feeding the microbiome: fiber. Studies have shown an increase in beneficial bacteria, like Bifidobacterium and Lactobacillus, in groups with high fiber diets compared to groups with placebo or low fiber diets.36 Fiber promotes a higher microbial diversity and microbiome resilience. Fruits and vegetables provide a variety of external microbes and probiotics. The combination of fiber and microbes contribute to a healthy gut microbiome. The shift from a non-Western diet to a Western diet has had drastic effects, including a loss of native bacteria strains and a fiber deficit. A Western lifestyle lacks essential components that contribute to a diverse microbiome that leads to long- and short- term health effects.37

The Relationship with the Mediterranean Diet
The Mediterranean diet is not a high carbohydrate diet that contains simply breads and pasta. The diet is composed of fresh fruit, vegetables, fish, whole meal cereals, beans and pulses (edible seeds of plants in the legume family), unsalted nuts and seeds, small amounts of lean meat and low fat dairy, olive oil, fresh herbs and wine.7 Food is not the only component of the diet. Conviviality, or the social aspect of eating, is an essential part alongside physical activity and a relaxed lifestyle. The Mediterranean diet contributes to improved metabolic health through the reduction of circulating bacterial endotoxins and diversity of the microbiota. Increasing levels of bacterial endotoxins have been proposed as a cause of inflammation during metabolic dysfunction.37
Numerous studies have confirmed the Mediterranean diet diversifies the gut microbiome. One study concluded that the diet increases the probiotic bacteria, Lactobacillus, when compared to the control group that was on a Western diet.13 Researchers replicated these findings in a study of Spanish men who ate a traditional Mediterranean-style diet. Study subjects had increased populations of Bifidobacterium and Lactobacillus. These bacterial species also had the ability to stimulate the growth of other beneficial bacterial species involved in methane and butyrate production.38
Feeding the human microbiota effectively requires microbiota- accessible carbohydrates (MACs). MACs are a primary source of energy for the microbiome and come from a fiber-rich diet. A MAC-rich diet has few simple sugars, unlike the typical Western diet, and its main contributor to the host metabolism is through small chain fatty acid fermentation of end products of the microbiota. The Western diet is low in MACs which results in a low microbiota diversity and metabolic output.12 Increases in mucus-utilizing microbes, slow gut motility, and increased calories from fat and sugars all contribute to cardiovascular diseases, obesity, and the deterioration of health.12
Dysbiosis, or microbial imbalance, contributes to the pathogenesis of intestinal and extra-intestinal disease. Inflammatory bowel disease can manifest within our intestinal tract due to dysbiosis.8 Allergies, asthma, metabolic syndrome, cardiovascular disease, and obesity occur outside of our intestines partly due to microbial imbalance.7 Avoiding dysbiosis can help to prevent some of these ailments. Hunter-gatherer diets promote a diverse microbiome since the diet is primarily based on fruits, vegetables, and high fiber content. The microbiome can ferment soluble fibers into short-chain fatty acids that are health- promoting and can help with metabolic syndrome.7
IMPLICATIONS FOR PHARMACY STAFF
Today, many healthcare providers steer patients toward a Mediterranean diet to improve cardio-metabolic issues. The American Heart Association devotes a page to the Mediterranean diet, noting that “Mediterranean diet” is a generic term for the typical eating habits in the countries that border the Mediterranean Sea.39 Healthcare organizations and advocacy groups use many different definitions, but often explain that this diet is based on whole or minimally processed foods. It includes many health-protective foods (fruits, vegetables, legumes, whole grains, fish and olive oil) and encourages patients to avoid adverse dietary factors (fast food, sugar-sweetened beverages, refined grain products, and processed or energy-dense foods). It also guides patients to limit red meat and alcohol intake, indulging moderately if at all.39,40
Pharmacy staff can be a resource for information about the diet, referring patients to local cooking classes or lectures that are given by health clinics. Most healthcare systems offer such classes to their patients and the community, and adult education programs often do, too. They can also target patients who have cardiovascular disease, diabetes, or renal failure for counseling, and steer them to discuss the Mediterranean diet with their health care professionals.
| Table 1. Resources for the Mediterranean Diet | |
| Oldways Cultural Food Traditions | ● Describes the Mediterranean diet, and also covers the principles and components of African, Asian, Latin, veg- an, and vegetarian diets
● Includes numerous recipes ● Provides links to advocacy groups and related programs |
| Mediterranean Diet 101: A Meal Plan and Beginner's Guide | ● Provides lists of foods, sample menus, and shopping lists
● Offers useful tips on eating out |
| What is the Mediterranean Diet?
https://www.cookinglight.com/eating-smart/nutrition- 101/what-is-the-Mediterranean-diet |
● Includes sample meal plans, recipe ideas, shopping lists
● Offers suggestions to add variety to meals |
| 22 Mediterranean Diet Recipes | ● A slideshow of recipes that incorporate the elements of an Italian or Greek diet |
Pharmacists and technicians should understand the diet and be able to answer questions about its health benefits. Hamilton Family Health Team offers a Mediterranean Diet Scorecard for free that emphasizes important points (https://hamiltonfht.ca/wp-content/uploads/Medi-Diet-Scoring-Tool.pdf) and is a handy tool for pharmacy staff. Pharmacies can also promote this diet annually in May, which is National Mediterranean Diet Month, with poster campaigns and information sheets.41 Table 1 provides additional resources.

CONCLUSION
It’s clear that diet has serious health implications. Astute readers probably noticed several things as they read. First, the Mediterranean diet emanates from food that the poor, working class people ate traditionally. It is based on healthy foods. Second, it’s highly probable that if researchers look at similar diets from other regions of the world, they would find similar health implications. (The authors assume you saw sauerkraut and kimchi listed in the fermented foods list in the Probiotics Sidebar, and reference to other old world diets in the Resources table.) Third, many readers may examine their own eating habits and see room for improvement.
Especially in occupations where long days, missed lunches, and consuming fast food quickly are the norm (do these things sound familiar?), convenience and processed foods may wiggle their way into many meals. Making good choices from foods included in the Mediterranean diet can improve overall health for patients and for pharmacists and technicians, too.