INTRODUCTION
Measles is an extremely contagious viral illness caused by an enveloped RNA virus of the genus Morbillivirus and family Paramyxoviridae.1,2 Once a routine childhood disease, the development and consistent administration of a measles vaccine effectually eliminated measles in the United States (U.S.). Recent falling vaccination rates have led to the reemergence of measles.3
Consider the following case: a man, Mike, and a toddler in a stroller, whose name is Bella, approach the pharmacy counter. He was shopping for nacho cheese flavored tortilla chips and saw the sign offering immunizations, which reminded him of his daughter’s recent well care visit. The pediatrician recommended routine vaccination with the measles, mumps and rubella vaccine, but Mike declined. He asks the pharmacist, someone he knows well and trusts, if the vaccine is necessary. Mike was under the impression there were no active measles cases in the U.S. Are there?
PREVALENCE
Prior to the availability of measles vaccine, almost everyone contracted measles during childhood. Approximately 90% of individuals obtained post-infection immunity by age 15.3,4
The Vaccination Assistance Act provided federal funding to state and local agencies for childhood immunizations beginning in 1962.5 In 1963, two measles vaccines became available in the U.S.: a single dose of a live attenuated vaccine or three once-monthly doses of an inactivated vaccine.6 The inactivated vaccine was eventually discontinued in 1967 because it was less effective than the live vaccine.6,7 By mid-1967, the reported number of measles cases had decreased from 1000 to 200 weekly.5
An increase in measles cases occurred from 1989 to 1991 due to decreased vaccination rates in young children and a rise in cases in individuals who had received only one dose of a measles vaccine. Increased vaccination awareness and rates in young children alongside the addition of a routine second dose of measles vaccine resulted in a major reduction in measles cases. The U.S. declared measles “eliminated” in 2000.1
PAUSE AND PONDER: What factors influence vaccination rates?
Since then, vaccine hesitancy due to misinformation regarding adverse effects and an incorrect association with autism has fueled decreasing vaccination rates. Other causes of declining measles vaccinations include missed routine vaccines during the COVID-19 pandemic and community complacency with measles’ severity and its complications. The resulting unvaccinated children are susceptible to the infection and its spread, thus propelling its resurgence.2,5
As of August 2025 in the U.S., 41 states had reported 1,356 confirmed cases of measles since January of that year. Most cases occurred in unvaccinated patients8:
- 92% were unvaccinated individuals or in people with unknown vaccination status
- 4% had received only one dose of MMR
- 4% had received two doses MMR.
Among these cases, 13% were hospitalized, and three cases resulted in death.8
A measles outbreak is defined as three or more related cases. From January to August 2025, the U.S. experienced 32 outbreaks, with 87% of confirmed cases related to these outbreaks. In 2024, 16 outbreaks were reported and 69% of measles cases were related to outbreaks.8
Reflecting on our case, the pharmacist explains to Mike that domestic cases are rising due to declining vaccination rates worldwide, and that vaccination offers the best protection available.
TRANSMISSION AND SYMPTOMS
Transmission of measles occurs by direct contact or airborne spread through respiratory droplets and aerosols, which can stay airborne for up to two hours in enclosed areas.1,5,7 About 90% of non-immune people who are exposed to the measles virus will become infected.7
The physical manifestation of measles infection begins 11 to 12 days after exposure with a prodrome of malaise, cough, coryza (runny nose and nasal congestion), and conjunctivitis.3 Approximately 50% to 70% of patients also develop Koplik spots, which are small white or grey papules in the mouth, during the prodrome phase.5
After two to four days, a red, macropapular rash (a flat, red area on the skin that is covered with small bumps that may merge together) occurs, usually on the face or hairline.3,9 The rash progresses to the trunk, and then to the lower extremities.3 Patients with uncomplicated measles usually improve by the third day after the rash began, and most cases resolve within seven to 10 days. Patients are contagious from four days before until four days after the onset of the rash.9
COMPLICATIONS
Complications of measles include diarrhea, dehydration, pneumonia, encephalitis, and death.3 For every thousand cases of measles, one case may lead to encephalitis and two to three cases may lead to death. Measles-related deaths are typically due to respiratory and neurologic complications.1,3
Rare complications of measles include measles inclusion body encephalitis (MIBE) and subacute sclerosing panencephalitis (SSPE). MIBE usually occurs in immunocompromised patients within one year of infection and is characterized by neurologic dysfunction, such as altered level of consciousness, seizures, loss of speech, one-sided paralysis, and lack of coordinated movements. MIBE has a mortality rate of 75%.1,10 SSPE is a degenerative central nervous system disease that results neurological decline and seizures. It usually develops seven to 11 years after infection, and it occurs most frequently in children infected with measles before age 2.1
Patients at higher risk for measles infection are unvaccinated or incompletely vaccinated, have had exposure to measles, or have traveled to areas with active measles.8
Severe cases of measles may require hospitalization.3 Patients who are younger than 5 or older than 20, pregnant, or immunocompromised are at the greatest risk for severe measles infections or complications.8
Back to our case: Mike asks if there is medicine Bella can take to speed up her recovery if she catches measles, rather than prophylaxis with a vaccine.
POST-EXPOSURE MANAGEMENT
Confirmation of Diagnosis
The diagnosis of measles is confirmed through laboratory findings. Positive serology for measles IgM antibodies, significant increase in IgG antibody levels, and cell culture of the measles virus can be assessed through blood assays. Evidence of measles RNA by reverse transcription polymerase chain reaction can be assessed through nasal, throat, or nasopharyngeal swab or a urine sample.5,11 Healthcare providers should obtain both a serum sample and a nasopharyngeal or throat swab or urine sample for all patients with clinical symptoms of measles.1,11 Just looking at the patient’s rash is not sufficient for diagnosis. Laboratory evidence is crucial because clinicians may incorrectly diagnose or report other febrile illnesses with rash as measles.5
Reporting to Health Department
Because measles has a significant impact on public health, it is a nationally notifiable disease. The purpose of national notification is to assess the incidence and spread of measles, with the goal of controlling outbreaks. Healthcare providers, laboratories, and hospitals should report confirmed cases of measles to local health departments. Each state has its own guidelines and requirements for reporting. The states report suspected and confirmed measles cases to the Centers for Disease Control and Prevention (CDC) using the National Notifiable Diseases Surveillance System.12,13
Post-Exposure Prophylaxis
Post-exposure prophylaxis (PEP) with measles, mumps and rubella vaccine (MMR) or immunoglobin in unvaccinated or partially vaccinated people may offer some protection against the disease, allowing for milder symptoms and a briefer course of illness.9 MMR should be administered within 72 hours of exposure.
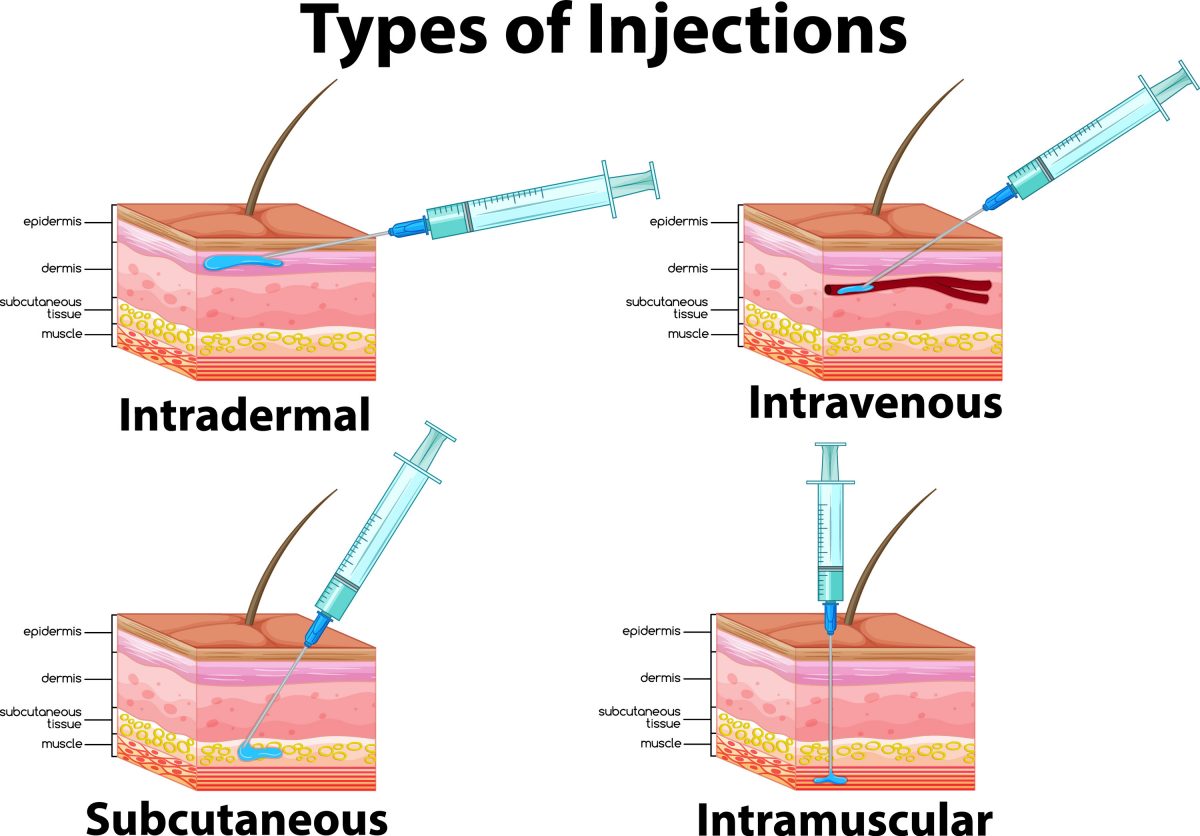
Patients who are ineligible for MMR (age less than 6 months, severely immunocompromised, or pregnant) and patients ages 6 to 11 months who did not receive MMR within the initial 72 hours can receive immunoglobulin within 6 days of exposure. Patients younger than 12 months of age can receive intramuscular immunoglobulin 0.5 mL/kg of body weight, with a maximum dose of 15 mL. Patients who are severely immunocompromised, pregnant, or weigh more than 30 kg can receive intravenous immunoglobulin 400 mg/kg.1
Patients should not receive both immunoglobulin and MMR because the immunoglobulin will decrease the vaccine’s efficacy.14 Patients without immunity who receive immunoglobulin should be given MMR or MMRV (MMR with a varicella component) at least 6 months after intramuscular immunoglobulin and 8 months after intravenous immunoglobulin.
Patients with documented immunity do not need PEP.1
Treatment of Measles
Treatment of measles is mainly limited to supportive care. Caregivers can give acetaminophen, ibuprofen, or intravenous fluids if needed for symptom control.15 Additionally, patients should isolate for four days after the rash appears to minimize the transmission of measles.16
No antivirals are currently approved by the Food and Drug Administration for the treatment of measles. Although the measles virus displays in vitro susceptibility to riboviran, this has not been studied in clinical trials and is not indicated for the treatment of measles.1
Treatment with vitamin A is an option for pediatric patients with measles. Vitamin A deficiency during measles infection has been linked with increased disease severity, additional complications, and prolonged recovery.15 Administration of vitamin A in children with measles in low- and middle-income countries has been connected to decreased morbidity and mortality.1 Although vitamin A deficiency is not as prevalent in higher income countries, infection with measles can reduce vitamin A stores.15 Given the benefit of vitamin A supplementation, the World Health Organization (WHO) recommends treatment with vitamin A for all children (not adults) with severe measles that requires hospitalization.1,15
Vitamin A is given once daily for two days, as described in Table 1. Additionally, a third dose of vitamin A should be given two to six weeks after the initial dose for children with signs and symptoms of vitamin A deficiency.1
| Table 1. Vitamin A Dosing1,15,17 |
| Age of child |
Dose: International Units (IU) |
Dose: retinol activity equivalent (RAE)* |
| 12 months or older |
200,000 |
60,000 |
| 6 to 11 months |
100,000 |
30,000 |
| Under 6 months |
50,000 |
15,000 |
| *Research at the turn of the Century found that provitamin-A carotenoid absorption is only half as much as previously believed. Consequently, the U.S. Institute of Medicine recommended a new unit, the retinol activity equivalent (RAE) in 2001. Each mcg RAE corresponds to 1 mcg retinol, 2 mcg of β-carotene in oil, 12 mcg of "dietary" β-carotene, or 24 mcg of the three other dietary provitamin-A carotenoids. |
Revisiting our case: the pharmacist explains to Mike that although treatment with vitamin A is an option that may ease severity and promote recovery, it will not treat the infection. Mike now shares that Bella received a single dose of MMR five months ago (at age 10 months) before a trip to Europe for his sister’s wedding. He is wondering why she would need to be vaccinated again. Doesn’t that dose offer protection?
VACCINE RECOMMENDATIONS
To be considered immune to measles, patients must have documented administration of an age-appropriate live measles containing vaccine, laboratory confirmation of either immunity or disease, or birth prior to 1957.3 Individuals born before 1957 are assumed to be immune to measles due to childhood exposure, as most people developed immunity through infection with the virus before the availability of the vaccine.5
Vaccination is key to measles prevention and control. Both the CDC and the American Academy of Pediatrics recommend routine vaccination with either MMR or MMRV.1,3 Table 2 provides additional information regarding current vaccines options.
| Table 2. Measles Vaccines Available in the United States1,18-20 |
| Brand name |
Manufacturer |
Active ingredients |
Age of administration |
Administration |
| M-M-R II |
Merck |
measles, mumps, and rubella vaccine, live
(MMR) |
12 months and older* |
0.5 ml subcutaneously or intramuscularly |
| Priorix |
GlaxoSmithKline |
measles, mumps, and rubella vaccine, live
(MMR) |
12 months and older* |
0.5 ml subcutaneously |
| ProQuad |
Merck |
measles, mumps, rubella, and varicella vaccine, live
(MMRV) |
12 months to 12 years |
0.5 ml subcutaneously or intramuscularly |
| *May be administered at ages 6 to 11 months for international travel, community outbreak, or post-exposure prophylaxis |
The first dose is usually given between 12 and 15 months of age, and the second dose is usually given between ages 4 and 6 years. The second dose may be given earlier, at least 28 days after the first dose for MMR and 90 days for MMRV, during a community outbreak of measles, before international travel, or to individuals who did not receive the vaccine during the recommended ages for administration. The MMRV vaccine should not be given to children younger than 1 year.1,21
The CDC recommends that MMR and varicella vaccines are given separately when administered as the first dose for children aged 12 to 47 months, unless the parent or caregiver prefers MMRV. Clinicians usually prefer MMRV as the second dose in children age 15 months to 12 years and for both doses in unvaccinated children age 48 months and older. The SIDEBAR explains this further.
At the time of this writing, the CDC Advisory Committee on Immunization Practices (ACIP) recommends that MMR and varicella vaccine be administrated separately until age 4. This is a change from the current recommendation to administer MMRV for the second dose in children 15 months and older. The ACIP recommendation is still pending approval from the CDC acting director and is not yet official.22
SIDEBAR: How to choose MMR vs. MMRV23
Piper, age 4, and her brother Oliver, age 12 months, are both due for measles and varicella vaccines. Piper received separate MMR and varicella vaccines when she was 1 year old. Their mom, Barbara, would like to minimize injections for each child. She asks if they can each receive MMRV to limit their shots today.
Although MMRV is indicated for children ages 12 months to 12 years, it has been associated with an increased risk of fever and febrile seizure when given as the first dose to children ages 12 to 47 months of age. Experts encourage healthcare providers to counsel parents and caregivers of children in this age group regarding the risks and benefits of MMRV vaccination. MMRV may be administered if the parent or caregiver prefers; however, the CDC recommends that MMR and varicella vaccines are given separately for the first dose in this age range.
Approximately 15% of children aged 12 to 47 months who receive MMR and varicella vaccines separately will experience post-vaccination fever (102°F or higher up to 42 days after vaccination), compared with 22% who receive MMRV. Administering the vaccines separately in this age group also decreases the febrile seizure risk by half: four of 10,000 children experience febrile seizure five to 12 days after vaccination with MMR and varicella separately, as compared to eight of 10,000 with MMRV.
For children aged 48 months and older, the risk of fever or febrile seizure with the first dose of MMRV declines and is similar to the risk when MMR and varicella vaccine are administered separately. The risk also decreases in all age groups when MMRV is administered as the second dose. Clinicians usually prefer MMRV for both doses in children aged 48 months and older and for the second dose in children ages 15 months to 12 years.
MMR and varicella vaccine should be administered separately for children with a personal or family history of seizures because they are at increased risk of febrile seizure after MMRV vaccination.
The pharmacist discusses the risks and benefits with Barbara, explaining that Piper received MMR and varicella vaccines separately at age 1 to reduce the risk of fever and febrile seizure. Because Piper is 4, she is an excellent candidate for MMRV. Barbara confirms that neither Oliver nor anyone in his family has a history of seizures. The pharmacist discusses the risks of MMRV at Oliver’s age (increased risk of fever and febrile seizures) and benefits (one injection rather than two). Barbara weighs the information presented to her and decides to follow the CDC recommendation of vaccinating Oliver with separate vaccines today, but will plan for MMRV for his second dose at age 4.
Before Barbara leaves, she pauses at the pharmacy counter. She asks about her niece, Lucy, who is 4 and unvaccinated. She wonders if Lucy is eligible for MMRV vaccination, and if consolidating shots might encourage Lucy’s mom to consider vaccination.
The pharmacist confirms that MMRV is appropriate for Lucy based on her age and vaccination status. Children aged 4 and older have not demonstrated an increased incidence of fever and febrile seizure when MMRV is administered as either the first or second dose. A decreased risk of adverse events and administration of a single injection rather than two with each dose may be preferable to Lucy and her parent. The pharmacist offers to contact Lucy’s mom and discuss vaccination options with her, explaining that Lucy could receive the first dose of MMRV now and the second dose in 90 days.
The MMR vaccine may be given to children ages 6 to 11 months if a community outbreak occurs or if the child is traveling internationally. For optimal efficacy, clinicians should give the vaccine at least two weeks before travel. It is important to note that a dose given before age 1 does not count towards completing the immunization series; a total of two doses are required to be administered after age 1, and doses given at ages 12 to 15 months and 4 to 6 years are still recommended.1
Reflecting back on our case: the pharmacist explains to Mike that Bella needs two doses after age 1 to ensure immunity to measles. Although Bella received a dose prior to international travel, she was younger than 12 months old, and it does not count towards completing the series.
PAUSE AND PONDER: Who else would benefit from measles vaccinations?
Although the guidelines are age based for routine administration, some patients may fall outside these parameters. Adults and older children, such as those in high school or college, who received a single dose after 12 months of age should receive a second dose, regardless of their current age.1
Other populations that should receive two doses of MMR, at least 28 days apart, include
- Students without immunity at educational institutions after high school, such as college or university
- International travelers without immunity
- Healthcare workers without immunity
- Healthcare workers born prior to 1957 without laboratory confirmation of immunity
- Close contacts of immunocompromised individuals who do not have documented immunity
- Individuals older than 12 months of age with human immunodeficiency virus (HIV) infection without immunosuppression and without immunity
An additional one to two doses of MMR may be required for 21
- Recipients of the inactivated measles vaccine between 1963 and 1967
- Individuals at risk during an outbreak as determined by a health department
People who should not receive MMR or MMRV are individuals with18-20
- Hypersensitivity to any component of a measles-containing vaccine
- Immunodeficiency or immunosuppression due to disease or medical therapy
- Pregnancy or those who plan to become pregnant within a month
- Active febrile illness with fever greater than 101.3°F (38.5°C) (M-M-R II and ProQuad)
- Active tuberculosis in those who are not receiving treatment (M-M-R II and ProQuad)
Patients who may be at greater risk for a experiencing a serious adverse reaction or having a less robust immune response after vaccination are those with21
- Acute illness, with or without fever
- Use of blood product containing antibodies within the past 11 months
- Thrombocytopenia or thrombocytopenic purpura
- Indication for tuberculin skin testing or interferon gamma release assay testing
- Seizures, either personal or family history
Back to the dad in our case: he’s still hesitant. He feels that his daughter has had so many vaccines already. And he’s read online that vaccines aren’t always safe. He wonders aloud if it is it really worth the risk?
VACCINE HESITANCY
Vaccine hesitancy (VH) is complicated and multifactorial. It is formed by social, cultural, political, and personal elements.24,25 The WHO defines VH as a “delay in acceptance or refusal of vaccines despite availability of vaccination services.”26 Examples include delaying vaccines, limiting the number of vaccines administered at the same time, avoiding specific vaccines, and omitting all vaccines completely.27 Some VH individuals believe that natural immunity (immunity resulting from infection) is more beneficial to the immune system than vaccine-induced immunity. While both routes provide immunity, the risks of vaccination are usually lower than the potential complications or consequences of acquiring the infection.25,28 VH is not clear cut; VH is a spectrum that encompasses a range of beliefs, attitudes, and actions.
PAUSE AND PONDER: How can pharmacy teams effectively address VH?
The 3 C model describes vaccine hesitancy as a result of decreased confidence, increased complacency, and decreased convenience. Table 3 describes the components of the 3 C Model of vaccine hesitancy.29
| Table 3. The 3 C Model of Vaccine Hesitancy29,30 |
| Confidence |
Patient trust regarding
• The safety and effectiveness of vaccines
• The healthcare system providing vaccines
• The motivation of policymakers who determine vaccine guidelines |
| Complacency |
• The risks of vaccine preventable diseases are believed to be low
• May occur when the disease being prevented is no longer prevalent |
| Convenience |
Ease in obtaining vaccination, influenced by
• Availability
• Affordability
• Accessibility
• Literacy
• Immunization services
• Comfort |
Healthcare providers might assume VH is a fairly new development, resulting from and driven by the Internet and social media. While it is true that social media often propagates vaccine misinformation, VH was first recognized more than 200 years ago with the administration of smallpox inoculation. VH evolved further in the late 1800s when smallpox vaccination requirements led to the adoption of personal belief exemption. Personal belief exemption, which is the practice of omitting a vaccination based on individual convictions, continued to gain popularity as more vaccines became available.24
Sources for vaccine information abound, including healthcare providers, the Internet, social media, word of mouth, and traditional media.27 Pharmacists are strong resources to answer vaccine questions and concerns because people view pharmacists as trusted and accessible. This position of responsibiliy allows pharmacists to help patients navigate the abundance of information—and misinformation—available.31
Traditionally, healthcare providers tackled individual VH through fact-based education to correct misinformation. However, a well-rounded approach focusing on individual beliefs in addition to evidence-based facts may be more effective in encouraging vaccine adoption.31
An option for addressing VH is the ASPIRE framework. This method helps pharmacists interact with patients regarding vaccination beyond basic education. It encourages pharmacists to actively engage with patients to establish trust and address their specific concerns.31
The ASPIRE framework consists of the following actions31:
- Assume that people want to be vaccinated and be prepared for questions
- Share key facts and information sources to counter misinformation
- Present strong recommendations to vaccinate and stories about vaccination experiences
- Initiate discussion or address questions about adverse effects proactively and share credible information sources
- Respond to questions and listen actively
- Empathize and understand concerns
In our case, the pharmacist recognizes Mike’s concern but assures him that misinformation is rampant. The pharmacist explains with empathy that measles vaccine is both safe and effective, and that exposure to the disease often carries severe complications. The pharmacist offers to vaccinate today. Mike decides to think it over while he shops for snacks. The pharmacist will continue to offer the vaccination every time Mike and Bella visit the pharmacy.
CONCLUSION
Measles is no longer a disease of the past. The recent uptick in cases is directly related to declining vaccination rates. Unvaccinated individuals are at risk for infection and complications, which may be severe. People without immunity may also transmit the disease to other unvaccinated individuals, perpetuating the cycle. Healthcare providers, laboratories, and hospitals should confirm suspected cases of measles with laboratory findings and report to the appropriate local health department. While supportive care may offer symptom control, prevention is key to measles control; both the MMR and MMRV vaccine are safe, effective, and available. Active and empathetic counseling techniques can help pharmacists build vaccine confidence and adoption.